

Abstract
INTRODUCTION
Good trunk performance is important for activities such as sitting and standing. In a cohort of patients with stroke, we sought to evaluate changes in trunk performance after stroke, establish factors correlated to trunk performance and assess the impact of trunk performance on discharge ambulatory and functional status.
METHODS
This was a retrospective review of the data of patients with stroke admitted to Tan Tock Seng Hospital rehabilitation centre, Singapore, over a two-year period. Data analysed included the National Institutes of Health Stroke Scale (NIHSS), Montreal Cognitive Assessment (MOCA), Fugl-Meyer Assessment (FMA) of limb motor impairment and Functional Independence Measure-motor (FIM-motor) scores, which measures self-care ability. Trunk performance was assessed on the Trunk Impairment Scale (TIS).
RESULTS
577 patients with stroke (mean age 63.2 ± 11.8 years) were analysed. Truncal impairment was present in 96.4% of patients. Mean admission TIS score was 14.3 ± 6.1 and this improved to 17.2 ± 5.2 on discharge (p < 0.001). Admission TIS score was positively correlated with admission MOCA, FMA-upper limb and FMA-lower limb scores, and negatively correlated to NIHSS score and neglect. Admission TIS scores significantly predicted discharge FIM-motor scores (p < 0.001) and ambulatory status (p < 0.001).
CONCLUSION
Truncal impairment was common and improvements in trunk performance were seen after rehabilitation. Trunk performance was significantly correlated to stroke severity, upper and lower limb motor power, cognition and neglect. As admission trunk performance predicted discharge functional and ambulatory status, it is recommended that trunk performance be evaluated for all patients with stroke.
INTRODUCTION
Good trunk performance is important for adequate performance of key activities such as sitting, standing and walking, as trunk muscles help to stabilise proximal body segments during voluntary movements of the extremities.(1) Selective movements of the trunk are also required to maintain the centre of mass within the base of support and to maintain an upright posture during shifting of weight. Clinically, trunk performance can be assessed by tests ranging from a simple assessment of the patient’s sitting balance to tests of balance (e.g. Berg’s Balance Scale(2)), and more structured and detailed truncal activities on a standardised scale, such as the Trunk Impairment Scale (TIS).(3) Previous studies have shown that impairments of trunk performance are common after stroke and they include impaired trunk muscle strength, decreased sitting balance and reduced truncal coordination.(1,4,5)
The importance of understanding trunk performance after stroke is underlined by the finding that it has been shown to predict the ability to perform activities of daily living.(6,7) In one study involving 102 patients with stroke, trunk performance on admission was even shown to be a stronger predictor of Barthel Index score at six months after stroke than that on admission.(8) These findings suggest that if trunk performance could be improved early in the rehabilitation process, better functional improvement after stroke might be possible. In a randomised controlled study of 33 patients with stroke, patients who received six hours of additional truncal exercises had significantly better truncal function, standing balance and mobility when compared to control patients.(9)
Less well studied is the recovery of trunk performance after stroke and the neurological impairments associated with trunk performance. The above has relevant implications for the timing of rehabilitation intervention and prognostication of patient outcome. In a small study involving 32 patients with stroke, the time course of recovery of trunk performance, as measured on the TIS, was similar to that of the arm and leg, with most recovery occurring within the first three months after stroke.(10)
At the Tan Tock Seng Hospital (TTSH) rehabilitation centre, Singapore, as part of our centre’s stroke database, we have been measuring truncal performance using the TIS for all patients with stroke admitted to the centre since 2014. This study on a cohort of patients with stroke admitted to our rehabilitation centre aimed to: (a) evaluate trunk performance before and after rehabilitation; (b) establish clinical factors associated with trunk performance; and (c) evaluate the impact of trunk performance on discharge ambulatory and functional status.
METHODS
All patients with stroke admitted to the rehabilitation centre at TTSH were prospectively included in the centre’s database. Admission to the centre’s stroke rehabilitation programme was evaluated by a rehabilitation physician and included the criteria: (a) significant impairment and disability that may improve with rehabilitation; and (b) ability to participate in at least two hours of therapy daily.
Data routinely captured in the centre’s database included: (a) measures of stroke-related severity and impairments, which included stroke severity as measured on the National Institutes of Health Stroke Scale (NIHSS),(11) cognition as assessed on the Montreal Cognitive Assessment (MOCA),(12) motor impairment as measured on the Fugl-Meyer Assessment (FMA)(13) and trunk performance as measured on TIS;(3) (b) functional status as measured on the Functional Independence Measure (FIM);(14) and (c) patient demographics, length of stay in rehabilitation and discharge disposition.
The TIS measured static sitting balance, dynamic sitting balance and coordination. Static sitting balance evaluated if a patient could keep a seated position, with both feet on the floor and their legs crossed. Dynamic sitting balance assessed selective lateral flexion, initiated from the shoulder and pelvic girdle. Finally, coordination evaluated selective rotation of the upper and lower part of the trunk against time. Scores of static sitting balance (range 0–7), dynamic sitting balance (range 0–10) and coordination (range 0–6) were summated to give total scores with a range of 0–23; the higher the score, the better the trunk performance. A score less than 23 suggested presence of truncal impairment. The TIS has been previously validated in patients with stroke.(3)
The FMA consisted of the FMA-upper limb and FMA-lower limb domains, and scores were in the range of 0–66 for FMA-upper limb and 0–34 for FMA-lower limb. Higher scores were associated with better motor power.
The FIM is a validated and reliable tool for assessing ability to perform self-care and mobility in various rehabilitation settings. It consists of 18 categories grouped into two subscales – motor and cognition. Each category scored in the range of 1–7; the higher the score, the more independent the patient was in performing the task associated with the item.
As the TIS was only routinely measured for all patients with stroke beginning in 2014, for the purposes of this study, only data of patients admitted in the years 2014 and 2015 was analysed. The inclusion criteria were: (a) patients with a first stroke (ischaemic and haemorrhagic) as diagnosed radiologically either on computed tomography and/or magnetic resonance imaging of the brain; and (b) admission to rehabilitation within four weeks of stroke onset. Exclusion criteria were: (a) patients with recurrent stroke; and (b) patients who did not complete their rehabilitation programmes.
FMA, FIM and TIS were assessed within 72 hours and one week of rehabilitation admission and discharge, respectively, while NIHSS and MOCA scores were only assessed on rehabilitation admission.
Statistical analysis was carried out using IBM SPSS Statistics version 22.0 (IBM Corp, Armonk, NY, USA). All statistical tests were carried out at a 5% level of significance, so that p < 0.05 was considered to be statistically significant. The t-test was used for comparison of means of continuous variables, Pearson correlation coefficient was used for correlation of continuous variables, and chi-square test was used for comparison of categorical variables.
The following analyses were performed: (a) comparison of TIS scores on admission to and discharge from rehabilitation; (b) correlation of measures of stroke severity and impairments with admission TIS scores; and (c) evaluation of the potential of admission TIS scores for predicting discharge ambulatory status and FIM-motor score.
The variables studied for correlation of measures of stroke severity to admission TIS scores included admission NIHSS, MOCA and FMA scores, neglect and age. Neglect was assessed based on relevant subscores of NIHSS and was defined as an NIHSS sensory extinction score ≥ 1.
Ambulatory status was assessed on the FIM-walk score. Poor ambulators were defined as patients with FIM-walk score ≤ 4 and good ambulators were patients with FIM-walk score ≥ 5. An FIM-walk score of 5 implied either that the patient required standby supervision, cueing or coaxing to go a minimum of 150 ft (50 m), or was able to walk only short distances (a minimum of 50 ft or 15 m) independently with or without a device.
For the prediction of discharge FIM-motor score, apart from admission TIS score, other variables analysed included age, neglect and admission FMA-total, NIHSS and MOCA scores. For (b) and (c), multivariate logistic regression analyses were performed if there were more than one significant independent variable on univariate logistic regression analysis.
The study was approved by the hospital’s ethics committee.
RESULTS
Data of 577 patients with stroke who met the inclusion and exclusion criteria was analysed. Clinical characteristics and rehabilitation outcomes are shown in
Table I
Clinical characteristics and rehabilitation outcomes (n = 577).
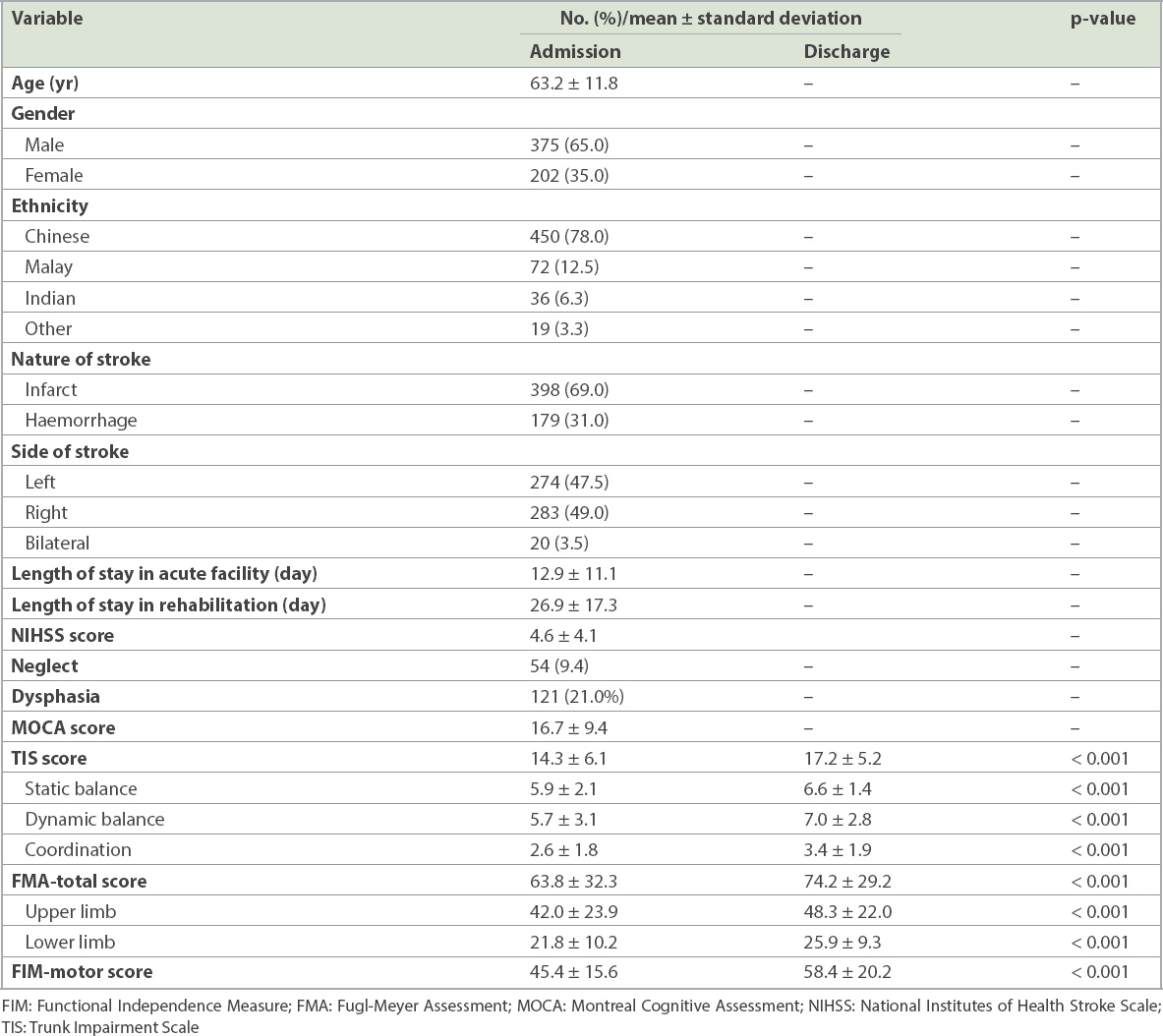
Only 21 (3.6%) patients had full TIS scores on admission, indicating that a majority of patients had impaired trunk performance. Mean change in TIS scores from admission to discharge was 2.8 ± 3.3 and this was statistically significant (p < 0.001). Significant improvements were also noted in all subscales of the TIS (p < 0.001). Patients with longer lengths of rehabilitation stay had significantly lower admission TIS scores (r = −0.45; p < 0.001).
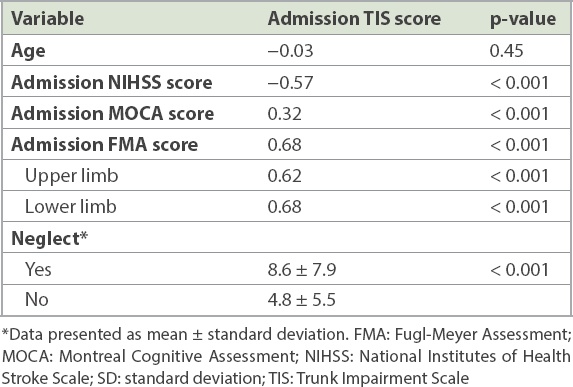
The results of analysis of variables associated with admission TIS score are given in
Table II
Univariate logistic regression analysis of variables associated with admission TIS scores.
Mean admission TIS score was significantly higher in patients with good discharge ambulatory outcome than in patients with poor discharge ambulatory outcome (16.5 ± 5.2 vs. 11.2 ± 7.3; p < 0.001). Median admission TIS score was 14, and the 25th and 75th percentile scores were 11 and 19, respectively. We compared the predictive potential of these different admission TIS scores and found the percentage of patients achieving good discharge ambulatory status with admission TIS scores ≥ 11, ≥ 14 and ≥ 19 were 63.9%, 68.8% and 72.3%, respectively. In the 21 patients with full admission TIS scores, 19 (90.5%) achieved good discharge ambulatory status.
Results of univariate logistic regression analysis of variables predicting discharge FIM-motor scores are shown in
Table III
Univariate logistic regression analysis of variables associated with discharge FIM-motor scores.
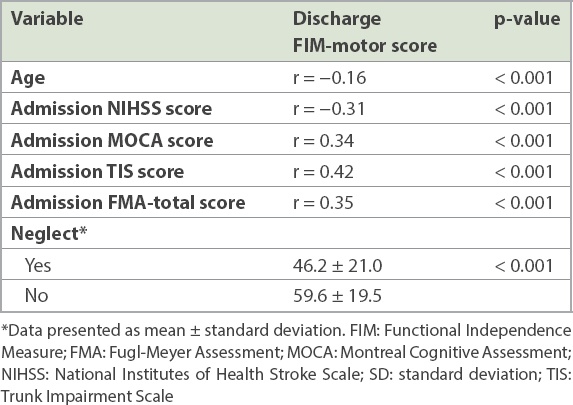
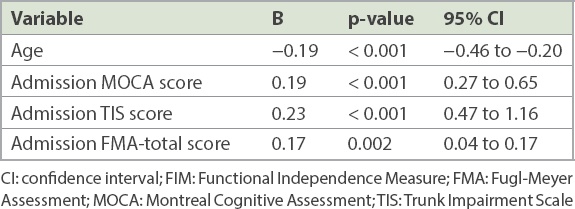
Table IV
Multivariate logistic regression analysis of variables associated with discharge FIM-motor scores.
DISCUSSION
In this retrospective study of 577 patients with stroke, impaired trunk performance was common, occurring in 556 (96.4%) patients. The relatively low mean admission TIS score of 14.3 suggested that most patients had significant truncal impairment. Breakdown of the admission TIS scores revealed almost full static sitting balance scores (mean score 5.9 out of a maximum score of 7) but low dynamic sitting balance (mean score 5.7 out of a maximum score of 10) and coordination (mean score 2.6 out of a maximum score of 6) scores. This was not surprising, as tasks on the last two subscales challenge the trunk more than tasks on static sitting balance.
Significant improvements in truncal performance were noted after rehabilitation, as evidenced by a mean gain of 2.8 ± 3.3 points on the TIS. This gain was very close to the minimal clinically important difference for TIS, which has been reported to be 3.5 in subacute stroke.(15) The number of patients, in our study, with a mean TIS gain of over 3.5 points was 160 (27.7%).
Admission TIS scores were significantly correlated to admission NIHSS, MOCA, FMA-upper and FMA-lower limb scores and neglect. Patients with lower admission TIS scores were more likely to have a severe stroke, cognitive impairment, greater upper and lower limb weakness, and neglect. Together, these factors accounted for 52% of variance of the admission TIS score. To the best of our knowledge, in the only previous study that looked at variables correlated to admission TIS score, van Nes et al reported that in a cohort of 78 patients assessed within two weeks of stroke onset, admission TIS score was independently correlated to age, limb motor power and neglect, and these three variables accounted for 65% of variance of the admission TIS score.(16) Patients in this earlier study were significantly older, with a mean age of 71.2 years, compared to 63.2 years in our study. This age disparity may explain why age was not a significant correlate of admission TIS score in our study.
The association between truncal impairment and upper and lower limb weaknesses has been reported previously. In a small study involving 32 patients with stroke from one week to six months after stroke onset, Verheyden et al showed that TIS score was closely correlated to upper and lower limb FMA scores at one week, one month, three months and six months after stroke onset, suggesting that truncal and limb recovery have similar recovery trajectories.(10)
Patients with neglect have decreased awareness of the affected side and this is associated with deviation of the trunk toward the affected side and, in some patients, contraversive pushing, a condition in which patients seem to actively push away from the non-paretic side.(17,18) Hence, the significant correlation between truncal impairment and neglect was not surprising. To the best of our understanding, cognitive impairment, as an independent correlate of truncal performance, has not been reported previously. One possible reason is that in some studies, patients with significant cognitive impairments were intentionally excluded out of concern about the ability of these patients to follow test protocols, which included performance on the TIS.(1,10,19) In our study, the TIS was performed on all patients, with or without cognitive impairment, and it was possible that those with significant cognitive impairments were more likely to be unable to follow instructions on the TIS, thus resulting in lower TIS scores. This could have possibly contributed to our finding of cognitive impairment as a significant correlate of trunk performance.
The finding that truncal impairment on admission was a significant predictor of discharge functional and ambulatory status was consistent with results of previous studies.(5-7,19,20) Patients with good discharge ambulatory status, on average, scored 5 points more on the admission TIS score when compared with poor discharge ambulators. The strength of admission TIS score in predicting discharge ambulatory status was also reflected in the finding that patients with admission TIS scores of 14 or higher had almost a 70% probability of achieving good discharge ambulatory status, and those with full admission TIS scores had a 90.4% probability of achieving good discharge ambulatory status. This information is particularly useful, as it helps guide patients and caregivers on the expected level of ambulatory status that could be achieved by the patient at the time of discharge and the need for continued ambulatory training.
As a predictor of discharge functional status, the admission TIS score was more important than other clinically relevant predictors, including age and limb motor power. This finding is of particular relevance, as recent studies have shown the positive impact of specific truncal exercises for improving trunk function, balance and mobility in patients with stroke.(9,21,22) Haruyama et al, in an assessor-blinded, randomised controlled trial of 32 participants in a stroke rehabilitation ward, showed that participants who received additional core stability training in lieu of conventional therapy had better scores on the TIS, Timed Up-and-Go test and Functional Ambulation Category.(22)
This study had several limitations. Firstly, patients in our cohort were selected for admission to rehabilitation based on their ability, and this selection bias limited the generalisability of our results. Secondly, the retrospective nature of the study meant that other clinical variables that may have potential impact on study outcomes (e.g. site of stroke and mood) could not be evaluated. Furthermore, as the NIHSS was measured on admission to rehabilitation rather than within 72 hours of stroke onset, it may not accurately reflect stroke severity, as NIHSS scores tend to improve over time. On the other hand, the study sample size of 577 patients is the largest of all existing studies investigating trunk performance in patients with stroke.
In conclusion, in this cohort of patients with stroke admitted to our rehabilitation centre, truncal impairment was common and improvements in trunk performance were seen after rehabilitation. Trunk performance was significantly correlated to stroke severity, upper and lower limb motor power, cognition, and neglect. As admission trunk performance predicts discharge functional and ambulatory status, it is recommended that trunk performance be evaluated for all patients with stroke and, in those with impaired trunk performance, truncal exercises be considered to optimise trunk performance.