

Abstract
INTRODUCTION
Unscheduled reattendances at the paediatric emergency department may contribute to overcrowding, which may increase financial burdens. The objectives of this study were to determine the rate of reattendances and characterise factors influencing these reattendances and hospital admission during the return visits.
METHODS
Medical records of all patients who attended the emergency department at KK Women’s and Children’s Hospital, Singapore, from 1 June 2013 to 31 May 2014 were retrospectively reviewed. We collected data on patient demographics, attendance data and clinical characteristics. Planned reattendances, recalled cases, reattendances for unrelated complaints and patients who left without being seen were excluded. A multivariate analysis was conducted to determine the odds ratio of variables associated with hospital admission for reattendances.
RESULTS
Of 162,566 children, 6,968 (4.3%) returned within 72 hours, and 2,925 (42.0% of reattendance group) were admitted on their return visits. Children more likely to reattend were under three years of age, Chinese, triaged as Priority 2 at the first visit, and were initially diagnosed with respiratory or gastrointestinal conditions. However, children more likely to be admitted on their return visits were over 12 years of age, Malay, had a higher triage acuity or were uptriaged, had the presence of a comorbidity, and were diagnosed with gastrointestinal conditions.
CONCLUSION
We identified certain subgroups in the population who were more likely to be admitted if they reattended. These findings would help in implementing further research and directing strategies to reduce potentially avoidable reattendances and admissions.
INTRODUCTION
The growing use of emergency departments (EDs) has raised the importance of reducing avoidable reattendances. Patients returning to the ED within 72 hours of their initial presentation may contribute to overcrowding,(1-4) which can lead to delayed treatment, patient dissatisfaction, straining of ED resources and increased healthcare costs.(1,2,5,6) Reattendances may be due to illness progression(3,7,8) or parental preference for ED care,(5) but may also reflect failure to appropriately diagnose, treat and communicate follow-up advice at the first visit.(2,3,7-9) In the paediatric population, parental concern or anxiety may play a significant role.(3,7,10) Higher reattendance rates may, therefore, indicate suboptimal clinical care or failure to address parental concerns at the first visit. Consequently, the incidence of unplanned reattendances is regarded as a quality-of-care indicator that drives the improvement of clinical care and communication delivered at the initial visit.(3,4,11,12) There is also an increasing focus on admissions for return visits, as high admission rates may represent medical errors such as misdiagnoses or inappropriate treatment.(8)
A majority of studies have associated reattendance with young age; higher acuity; attendance during the busiest hours; presence of chronic illness; infectious disease or respiratory diagnoses; and higher rates of admission.(1-3,7,9,13) In particular, children with chronic diseases have complex multidisciplinary care needs and may present to the ED more frequently when alternative sources of care are not available.(14-16)
In the present study, our primary objective was to determine the rate and characteristics of reattendances at our paediatric ED within 72 hours from the first visit. Our secondary objective was to identify demographic and clinical factors that may influence admission rates of reattendances. Factors of particular interest include patient age, time of initial presentation, triage acuity level, presence of comorbidities and diagnoses. Through this study, we hope to identify underlying factors associated with unplanned reattendances and thereby aid the implementation of strategies to address overcrowding, improve communication and, ultimately, enhance patient care.
METHODS
The emergency department at KK Women’s and Children’s Hospital (KKH), the largest tertiary paediatric emergency department in Singapore, is open to any child younger than 16 years of age. We reviewed electronic medical records of all patients who reattended the KKH paediatric ED within 72 hours from 1 June 2013 to 31 May 2014. Planned reattendances, recalled cases, reattendances for unrelated complaints and patients who left without being seen were excluded. Data was extracted from the ED’s electronic medical database, Online Paediatric Emergency Care (OPEC). Data collected included: (a) patient demographics (age, race and gender); (b) attendance data (time of the first visit, acuity at the first and return visits, duration between the first and return visit, and level of seniority of the attending physician during the first visit); and (c) clinical characteristics (type of comorbidity, diagnoses at the first and return visits, and disposition at the return visit). The study was approved by the SingHealth Centralised Institutional Review Board.
The ED at our institution uses the Singapore Paediatric Triage scale, a four-level triage system that categorises patients into four priority categories: Priority 1, Priority 2 Plus, Priority 2, and Priority 3. Priority 1 refers to emergent cases that require immediate attention and may involve resuscitation. Priority 2 and 2 Plus refer to urgent cases that may deteriorate if not seen quickly; specifically, Priority 2 Plus cases require medical attention within ten minutes from the time of arrival at the ED. Priority 3 refers to nonurgent cases. Time of visit was defined as the time of registration during the first visit to the ED, classified as morning (8.30 am–4.30 pm), evening (4.30 pm–11 pm) or night (11 pm–8.30 am) based on the shift hours of the staff. The duration between the first and return visits was divided into: (a) ≤ 24 hours; (b) > 24 hours but ≤ 48 hours; (c) > 48 hours but ≤ 72 hours; and (d) more than one return visit within a 72-hour period.
The comorbidities and diagnoses were classified according to the International Classification of Diseases, 10th revision.(17) Each patient was reviewed by an attending physician whose seniority was classified as follows: a senior doctor is a trained specialist registrar and above; a resident doctor is enrolled in a training specialist programme (including paediatrics, emergency medicine and family medicine); and a non-resident doctor is not enrolled in a training specialist programme.
Statistical analysis was carried out using Microsoft Excel (Microsoft Corp, Redmond, WA, USA) and IBM SPSS Statistics version 19.0 (IBM Corp, Armonk, NY, USA). Categorical variables were compared using chi-square test and continuous variables using Student’s t-test. A multivariate logistic regression model was developed to estimate the odds ratio (OR) for factors that influenced admission rates for ED reattendances. Adjusted ORs were expressed with 95% confidence interval and statistical significance was set at p < 0.05. Variables used in our multivariate logistic regression model included ED reattendance, age, gender, race, staff shift at time of visit, initial diagnosis, presence of comorbidity, doctor’s level of seniority and triage acuity level.
RESULTS
In the one-year study period, there were a total of 171,112 attendances at the ED involving 162,566 patients. 6,968 patients (4.3%) reattended the ED within a 72-hour period and 155,598 patients did not reattend. On the return visit, of the 6,968 patients who reattended, 3,983 (57.2%) were discharged, 2,925 (42.0%) were admitted and 60 (0.9%) were discharged against medical advice. Of those who were discharged, 874 (21.9%) patients were given a follow-up appointment and 3,109 (78.1%) were not.
Fig. 1
Flowchart shows the reattendance visits, exclusion criteria and final disposition of patients who reattended the emergency department from 1 June 2013 to 31 May 2014. Exclusion criteria included planned reattendances (i.e. reviews for neonatal jaundice and dengue), recalled cases, reattendances for unrelated complaints and patients who left without being seen. AOR: discharged against medical advice.
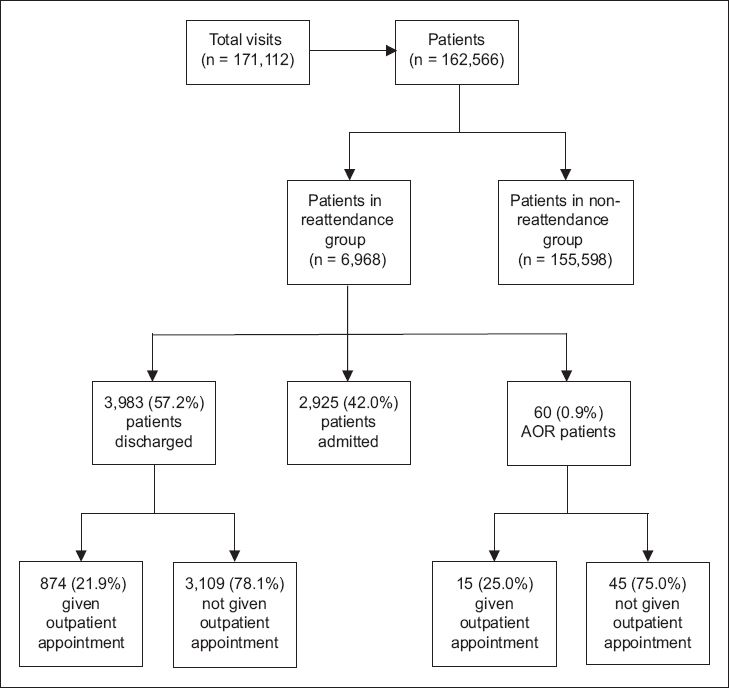
Table I
Demographic and clinical characteristics by emergency department reattendance within 72 hours.
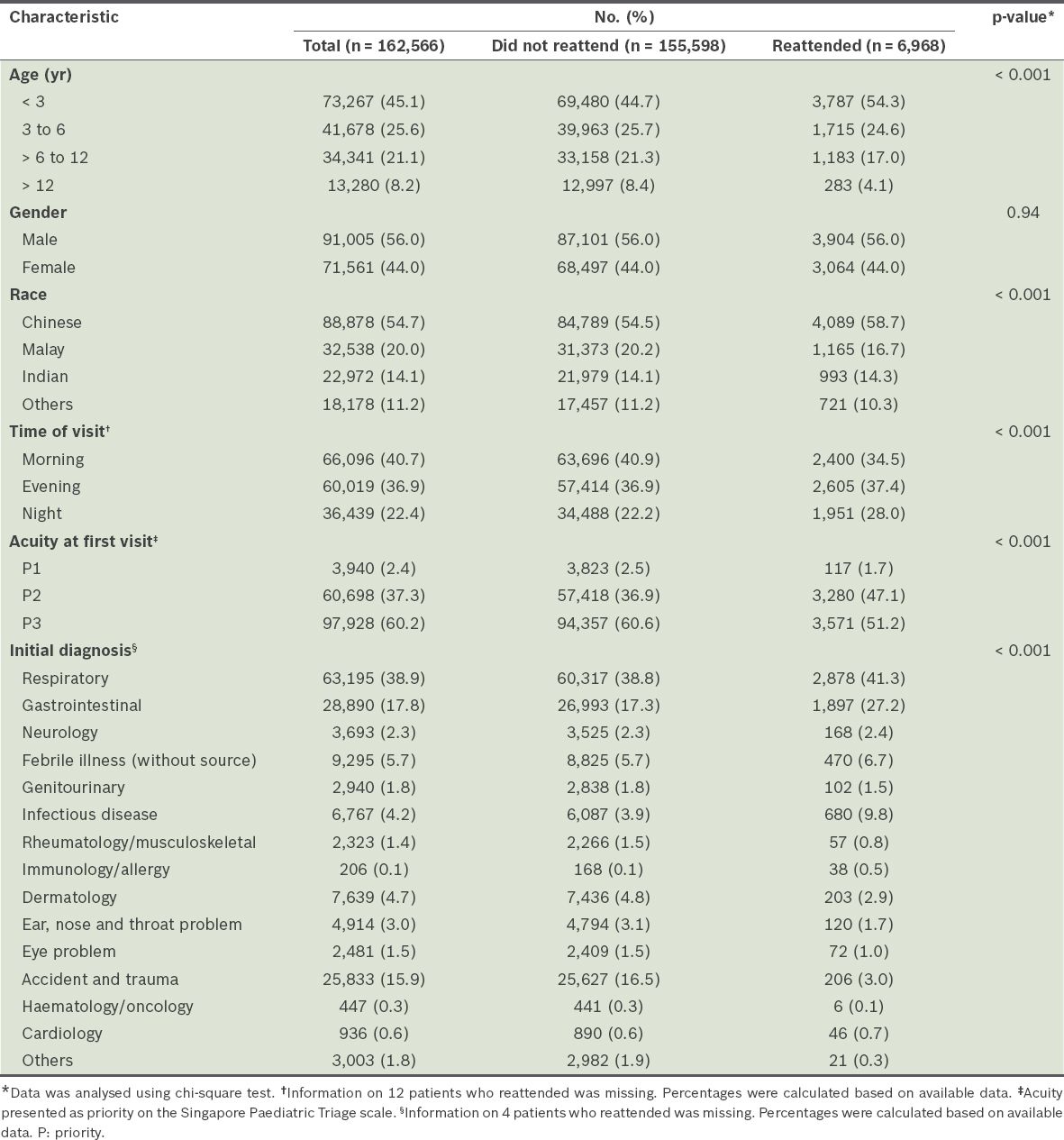
Table II
Demographic and clinical characteristics by emergency department (ED) admission at reattendance (n = 6,908).
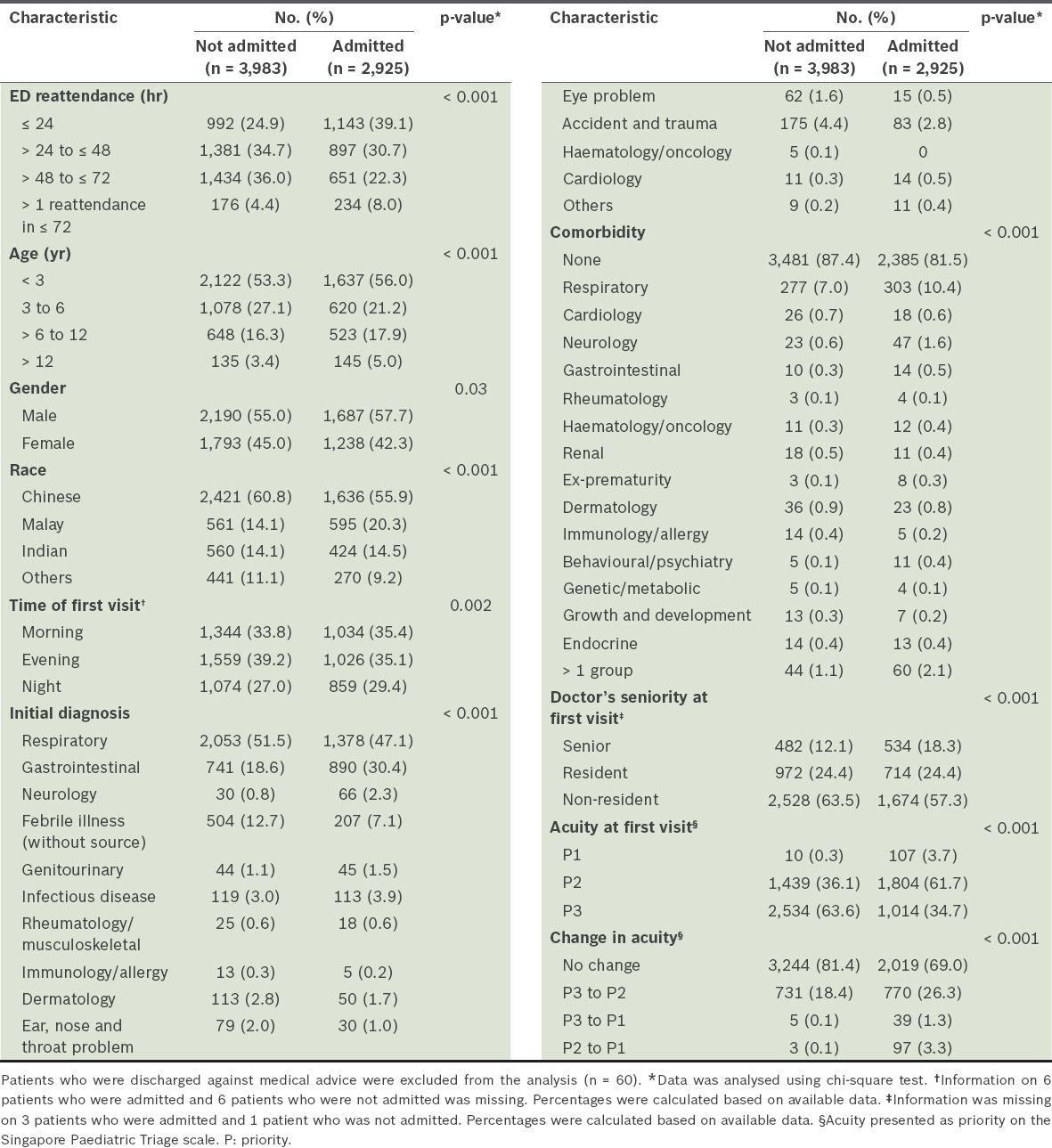
Table III
Multiple logistic regression analysis of the characteristics of patients who were admitted at reattendance.
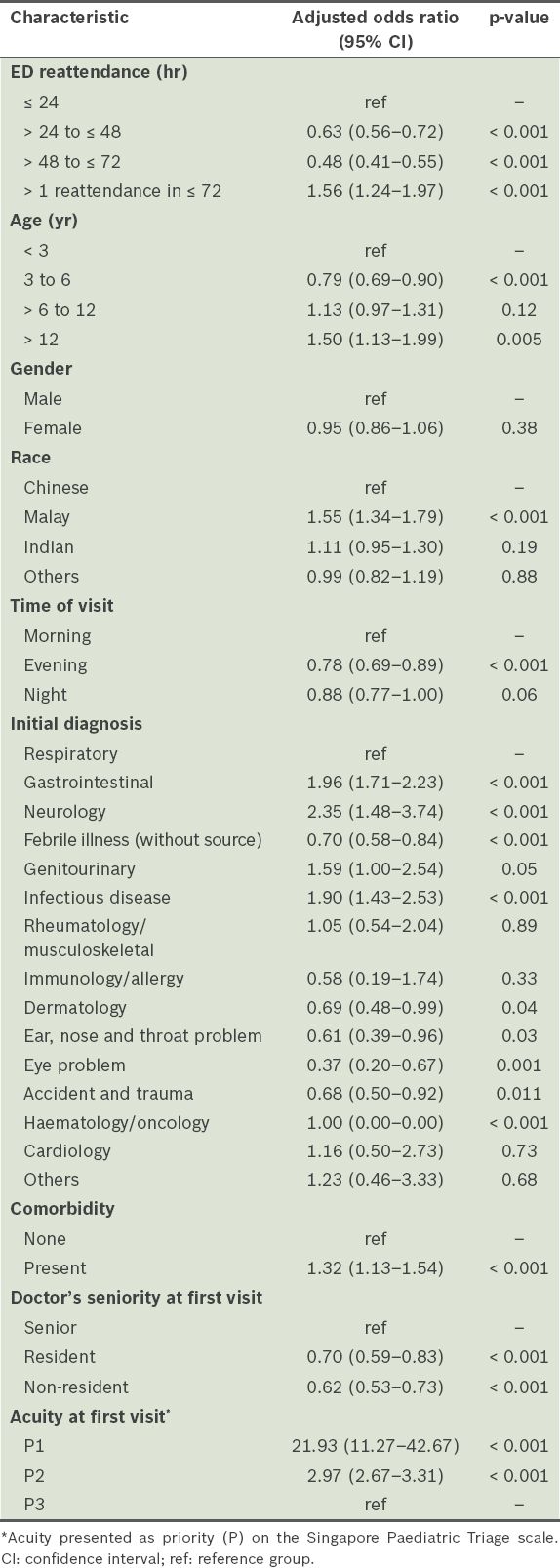
Children under three years of age represented the largest proportion of all ED visits (45.1%) and reattendances (54.3%). However, children over 12 years of age were more likely to be admitted on their return visits when compared to those under three years of age (OR 1.50, CI 1.13–1.99; p = 0.005). The racial distribution of patients attending our ED was comparable to that of the general population.(18) Malay children were more likely to be admitted on return visits compared to Chinese children (OR 1.55, CI 1.34–1.79; p < 0.001). Priority 2 patients were more common among patients who reattended than among those who did not reattend (47.1% vs. 36.9%; p < 0.001). In addition, patients who were initially triaged as Priority 1 and Priority 2 cases were more likely than Priority 3 cases to be admitted on their return visit (p < 0.001). 23.8% (n = 1,645) of reattendances had a change in triage acuity, of which 91.2% (n = 1,501) were uptriaged from Priority 3 to Priority 2. Of note, there were 44 patients who were uptriaged from Priority 3 to Priority 1, which was 0.6% of the total patients who reattended. Multiple reattendances within 72 hours were more likely to be associated with admission on the return visit than single reattendance within 24 hours (OR 1.56, CI 1.24–1.97, p < 0.001). Among patients who reattended within 24 hours, a significantly higher proportion were admitted than discharged (39.1% vs. 24.9%; p < 0.001).
Most reattendances were seen by non-residents (60.9%, n = 4,202) in the first visit, followed by residents (24.4%, n = 1,686) and senior doctors (14.7%, n = 1,016). Children attended to by a resident or a non-resident doctor during the first visit were less likely to be admitted compared to those attended to by a senior doctor (p < 0.001). 15.1% (n = 1,042) of the reattendance population had one or more comorbidity; respiratory comorbidities were most frequently observed. The presence of comorbidities was significantly associated with hospital admission (OR 1.32, CI 1.13–1.54; p < 0.001).
Respiratory and gastrointestinal diagnoses were the two most common diagnoses in both overall ED attendances (38.9% and 17.8%, respectively) as well as reattendances (41.3% and 27.2%, respectively). In the reattendance population, patients with gastrointestinal diagnoses were more likely to be admitted (OR 1.96, CI 1.71–2.23; p < 0.001) compared to those with respiratory diagnoses. Accident and trauma diagnoses accounted for only 3.0% of reattendances despite being the third most common diagnosis for overall ED visits.
DISCUSSION
With rising ED attendance rates, there has been a growing need to address the issue of overcrowding.(19,20) Analysing factors associated with reattendances may aid in reducing potentially avoidable ED reattendances, and in turn reduce financial and healthcare burdens.
The present study found that the reattendance rate was 4.6% within a 72-hour period from the first ED visit. This was consistent with the average rate of 5% reported in previous studies.(1) It has been reported that the rate of unplanned reattendances may reflect the quality of care provided by the ED. Our reattendance rate was well within the limits set by the American Academy of Paediatrics as well as the Department of Health in the United Kingdom.(21)
In addition, the admission rate among reattendances was 42.0%. This was higher than the overall admission rate of 16.5% among ED patients at our institution over the same duration, which is a trend seen in most other EDs.(2,3,7) Physicians may be more inclined to order additional investigations or have a lower threshold to admit patients at the return visit.(3) For the paediatric population, parental anxiety plays a major role in influencing the disposition of the child.(7)
The patient’s age was found to be inversely proportional to the reattendance rate at our ED, consistent with preceding studies.(1,7,9) Young patients are often unable to express their discomfort, leading to ambiguity in signs and symptoms. Parents, especially first-time parents, may also have a lower threshold to revisit the ED for any change in symptoms or concerns in younger patients. Interestingly, we found that patients over 12 years of age were more likely to be admitted on their return visits compared to those aged under three years. Cho et al(3) previously suggested that adolescents, as well as very young children, were more likely to revisit the ED. The present study showed that adolescents were less likely to revisit the ED, but were more likely to be admitted on their return visits. This could be related to their noncompliance to treatment or follow-up appointments. It may also reflect the higher tendency of true illness progression in adolescents compared to younger children, whose return visits may largely be influenced by parental anxiety. It may be worthwhile analysing this subgroup of patients to determine potential contributing factors that may influence admission rates.
Compared to patients of other races, the Malay patients in our study were more likely to be admitted on their return visits, possibly reflecting a higher incidence of chronic diseases and increased reliance on the ED for routine care. In addition, language barriers may impair understanding of discharge instructions, or limit accessibility to primary care resources.(22,23) Previous studies have also identified differences in healthcare-seeking behaviours and medical care among various ethnic groups.(14,23-26) Future interventions could include employing medical interpreters in the ED as well as improving accessibility to primary paediatric care in the community.
In terms of attendance characteristics, patients with a higher acuity level at initial triage were more likely to be admitted on the return visit, a trend clearly established in preceding studies.(1,13,22) High-acuity patients are generally more unwell and may have returned because of illness progression.(13) 91.5% (n = 107) of patients who were initially triaged as Priority 1 cases subsequently required admission. Uptriaging of acuity was also significantly associated with higher admission rates. These patterns should prompt clinicians to consider early admission in higher-acuity cases. It is important to consider illness progression as an underlying cause of the increased rates of admission for children returning to the ED within 24 hours. This may be particularly true for children with respiratory conditions, as they may deteriorate within a short period.(27,28) On the other hand, parental anxiety and increased pressure on the physician may account for the higher likelihood of admission of children who reattended multiple times.
Most of the reattendances were seen by non-resident doctors during the initial visit, a trend that reflects the general staffing distribution at KKH. Consulting a doctor of greater seniority at the first visit was notably associated with a greater likelihood of subsequent admission. This may partially be attributed to the fact that higher acuity cases are often assigned to senior doctors.(13) However, the association persisted even after adjusting for triage acuity level. Another postulation was the varying degree of safety netting advice given, as delivering clear and targeted advice ensures that patients with illness progression return in a timely manner.(29) At the same time, other studies have shown that the level of training of the primary doctor was not significantly associated with admission rates.(13,30,31)
The presence of comorbidities was independently associated with higher likelihood of being admitted at reattendances, notably for respiratory comorbidities. Hence, healthcare institutions may wish to consider focusing interventions on respiratory conditions and increasing accessibility in the primary outpatient setting. Respiratory diagnoses were also reported as the most common diagnoses during return visits in other studies.(9) This was not unexpected, as respiratory conditions have the potential to deteriorate more rapidly. However, we found that patients diagnosed with gastrointestinal complaints were more likely to be admitted compared to respiratory diagnoses, and the underlying cause and significance requires further investigation.
Being the largest tertiary paediatric hospital in Singapore, KKH was well-equipped to obtain a large sample size. Therefore, although our study was conducted at only one centre, we believe that the sample is representative of the country’s paediatric population. Nevertheless, as this retrospective study relied on accurate data collection and documentation, interpretation may have been limited by information bias. Another limitation was the role of confounding factors, which was minimised by the use of multivariate logistic regression.
This study did not examine the association of reattendance rates with health insurance or caregiver-related factors, such as parental age and the level of parental education. Public insurance has often been associated with a higher reattendance rate compared to private insurance.(3,9,13) Parental patterns of healthcare use have also been shown to influence the use of ED visits for their children.(32) Efforts to educate parents may potentially reduce the reattendance rate.
An earlier survey exploring reasons for nonurgent paediatric ED attendances at our ED found that most caregivers visited out of convenience, seeing it as a one-stop centre for care.(33) Other reasons cited included parental perception of the urgency of an illness and lack of confidence in caring for a sick child. This survey can be extended to investigate reasons for ED reattendances.
KKH has a pre-existing dial-a-nurse service that is open to all parents. The feasibility of expanding the current service to include diversion of ambulance calls should be explored, as studies have shown that diverting emergency calls to a call-in nurse service may potentially reduce the number of ED attendances without increased adverse outcomes.(34-36) Similarly, follow-up calls to subgroups of patients identified as having high reattendance rates, such as the young population in the present study, may help address parental concerns and alleviate the burden of ED reattendance. However, current studies have not demonstrated a reduction in reattendance rates in the paediatric ED(37,38) and the practicality of such a strategy remains questionable.
Primary care plays an important role in reducing nonurgent attendances at the ED, but its accessibility may be limited after office hours.(39-42) Studies have shown that introducing 24-hour primary care services led to a reduction in paediatric ED visits, particularly in nonurgent cases.(43) Maintaining continuity of care with primary physicians may also reduce rates of admission for children with comorbidities.(44) The importance of a primary physician for the adolescent population should also be reiterated, as this population has been identified as being at risk of readmission.
Observation units have been implemented in various paediatric EDs in countries such as Australia and the United States. They may facilitate closer monitoring of illness progression and increase parental satisfaction, thereby leading to a reduction in reattendance rates as well as avoidable admissions.(45-47) Short-stay observational units are particularly helpful in reducing reattendance rates for children with respiratory and gastrointestinal complaints, which were identified in our study as the most common return visit diagnosis and readmission diagnosis, respectively.
In conclusion, this study is one of the first to analyse reattendances at the paediatric ED in an Asian population. Our reattendance rate shows the quality of care delivered at the ED. We identified higher admission rates in children who were over 12 years of age, Malay, triaged as higher acuity cases and had gastrointestinal diagnoses. These findings would aid in implementing further research as well as directing future strategies to reduce potentially avoidable reattendances and admissions.