

Abstract
INTRODUCTION
Knowledge of morphological variations of the suprascapular region is important in the management of entrapment neuropathy and interventional procedures. The objective of this study was to collect data on the morphological features and dimensions of ossified ligaments and unusual bony tunnels of scapulae from a North Indian population.
METHODS
A total of 268 adult human scapulae of unknown gender were obtained from the bone bank of the Department of Anatomy, Dayanand Medical College and Hospital, Ludhiana, Punjab, India. The scapulae were evaluated for the incidence of ossified superior transverse scapular ligaments (STSLs), ossified inferior transverse scapular ligaments (ITSLs) and bony tunnels (i.e. the bony canal between the suprascapular notch and spinoglenoid notch), found along the course of the suprascapular nerve (SSN). The dimensions of these structures were measured and noted down. Ossified STSLs were classified based on their shape (i.e. fan- or band-shaped) and the dimensions of the ossified suprascapular openings (SSOs) were measured.
RESULTS
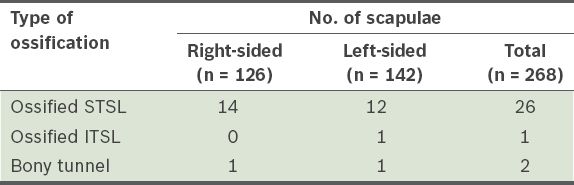
Ossified STSLs were present in 26 (9.7%) scapulae. Among the 26 scapulae, 16 (61.5%) were fan-shaped (mean area of SSO 16.6 mm2) and 10 (38.5%) were band-shaped (mean area of SSO 34.2 mm2). Bony tunnels were observed in 2 (0.75%) specimens, while an ossified ITSL was observed in 1 (0.37%) specimen.
CONCLUSION
The data obtained in the present study augments the reference literature for SSN decompression and the existing anatomical databases, especially those on Indian populations. This data is useful to clinicians, radiologists and orthopaedic surgeons.
INTRODUCTION
Knowledge of anatomical variations and anomalies along the course of the suprascapular nerve (SSN) is important in the treatment of SSN entrapment syndrome, and bony and brachial plexus injuries. This knowledge is also important for surgeons carrying out surgical interventions at the shoulder region.
The SSN provides sensory innervation to the posterosuperior aspect of the shoulder and motor innervation to the supraspinatus and infraspinatus muscles. The SSN passes beneath the superior transverse scapular ligament (STSL) and inferior transverse scapular ligament (ITSL) at the fibro-osseous canals of the suprascapular notch and spinoglenoid notch, respectively. Therefore, the STSL and ITSL are potential sites of SSN compression. Complete ossification of the STSL with formation of bony foramina is the most recognised predisposing factor for compression at the suprascapular notch;(1) it is also a risk factor in surgical exploration for SSN decompression.(2)
In a recent histological and immunohistochemical study, it was found that all five cadaveric shoulders that had STSL ossification showed signs of neural degeneration in the nerve specimens.(3) However, a high incidence of ossified STSL does not proportionally correlate with the occurrence of SSN entrapment;(4,5) this could be due to the lack of focus on the influence that the body ridge shape (created by the ossified STSL) has on SSN entrapment. With this in mind, the present study was designed to analyse the variable morphological aspects of the ossified STSL, along with other ossified ligaments found in the scapula. We also document any rare findings of ossified ITSL and bony tunnels (i.e. the bony canal found between the suprascapular notch and spinoglenoid notch), as well as their dimensions, as these structures could potentially compress vascular and neural elements by reducing available space in the spinoglenoid notch.(6,7)
In short, the present study explored the incidence of ossified ligaments and bony tunnels along the course of the SSN in dry human scapulae from a North Indian population. We also measured and recorded the dimensions of osseous ligaments and any rare bony tunnel and foramina at the suprascapular notch and spinoglenoid notch. As the existing data on ossified ligaments of dry human scapulae is limited, the data obtained in the present study would augment the current anatomical and morphological reference values. This would also aid in defining the anatomical risk factors for SSN entrapment and identifying the surgical hazards present during open and arthroscopic interventions in the suprascapular and spinoglenoid notch regions.
METHODS
The present study was conducted on 268 dry human adult scapulae of unknown gender from a North Indian population. Among the 268 scapulae, 126 were right-sided and 142 were left-sided. The specimens were obtained from the bone bank of the Department of Anatomy, Dayanand Medical College and Hospital, Ludhiana, Punjab, India. Scapulae with ossified ligaments along the course of the SSN were identified and their morphological variations studied in detail. The ossified ligaments were classified into: (a) ossified STSL – the bony bridge that converts the suprascapular notch into an osseous foramen; (b) ossified ITSL – the bony bridge that converts the spinoglenoid notch into an osseous foramen; and (c) bony tunnel – the ossified sheet posterior to the root of the coracoid process that forms a tunnel between the suprascapular notch and spinoglenoid notch.
The morphological parameters of the ossified ligaments were measured and recorded, along with the dimensions of the bony foramina that were formed by the ossified ligaments. The ossified STSLs were further classified into two groups – fan-shaped or band-shaped – based on the relative ratio of their proximal and distal widths (Figs.
Fig. 1
Photographs show the dorsal aspect of two dry scapulae, with a (a) fan-shaped ossified superior transverse scapular ligament (STSL) and a (b) band-shaped ossified STSL. The proximal width (PW) of the fan-shaped scapula is larger than its distal width (DW), whereas the PW and DW of the band-shaped scapula are almost equal. L: length of ossified STSL
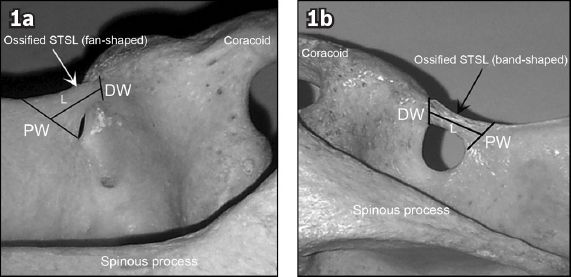
Fig. 2
Photograph shows the top view of a left scapula that has an ossified inferior transverse scapular ligament (ITSL). The measurements taken for an ossified ITSL are shown. DW: distal width; L: length of ossified ITSL; PW: proximal width
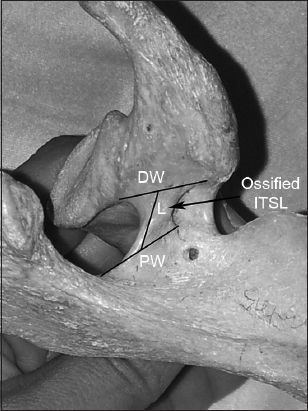
Fig. 3
Photograph shows the dorsal view of an ossified suprascapular opening (SSO) and the measurements taken. HD: horizontal diameter; STSL: superior transverse scapular ligament; VD: vertical diameter
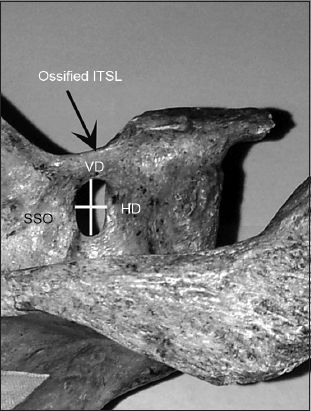
Fig. 4
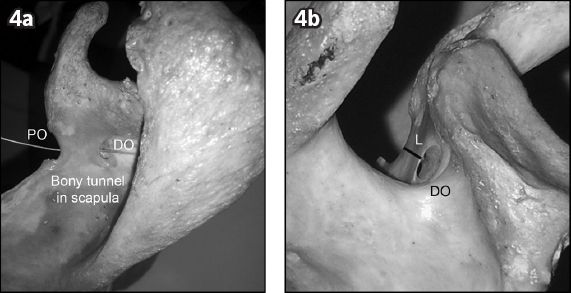
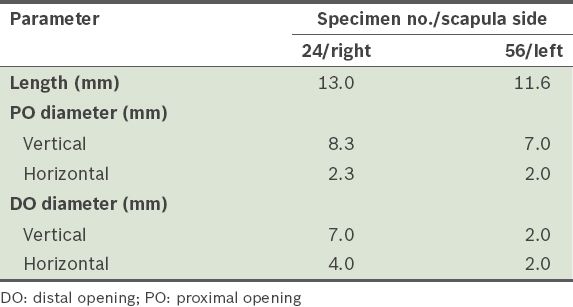
Photographs show (a) the superior view of a right scapula, with a probe passing through the bony tunnel, which is located between the supraspinous notch and spinoglenoid notch; and (b) the end-on view of the bony tunnel as seen from the spinoglenoid notch to show the distal opening (DO). L: length of bony tunnel; PO: proximal opening
RESULTS
Among the 268 scapulae studied, ossified STSLs were found in 26 scapulae, ossified ITSLs were found in one scapula and bony tunnels were found in two scapulae (
Table I
Frequency of ossified superior transverse scapular ligament (STSL), ossified inferior transverse scapular ligament (ITSL) and bony tunnels.
There was a greater prevalence of fan-shaped ossified STSLs (n = 16) than band-shaped ossified STSLs (n = 10). Among the fan-shaped ossified STSLs, there was an equal incidence of right and left scapulae (n = 8 each). Band-shaped ossified STSLs were more commonly found on right scapulae (6/10). The mean proximal width and length of fan-shaped ossified STSLs were greater than those of band-shaped ossified STSLs (
Table II
Measurements of the two types of ossified superior transverse scapular ligament (STSL) (n = 26).
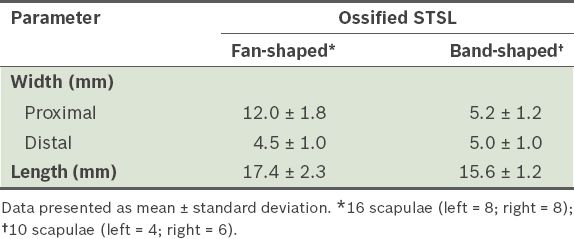
Table III
Measurements of ossified suprascapular openings (SSOs) in the two types of ossified superior transverse scapular ligaments (STSLs).
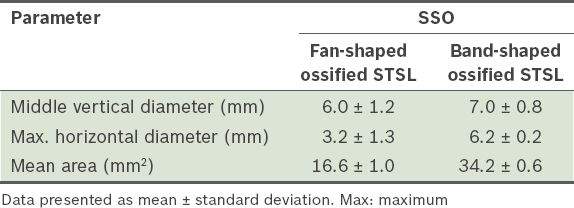
Table IV
Measurements of the bony tunnels (n = 2).
DISCUSSION
Ossification of the STSL results in the suprascapular notch being converted into a foramen. Various authors have reported the presence of such foramina in different population groups.(8-17) The results of the present study suggest a higher incidence of ossified SSOs in North Indian populations (
Table V
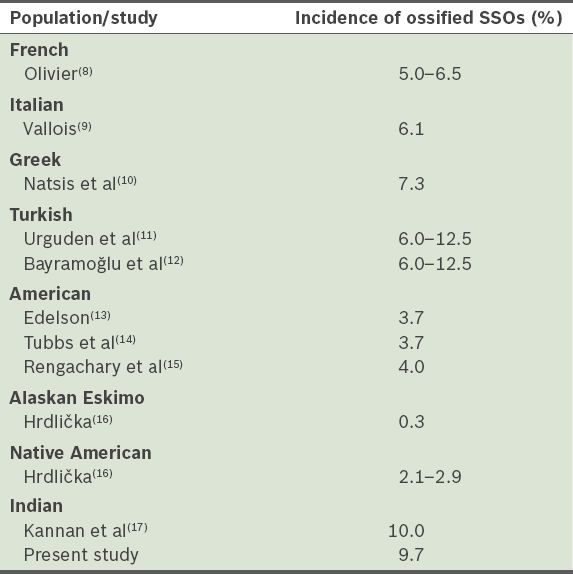
It has been suggested that variations in the appearance of an ossification centre for the coracoid and its associated bone formations may account for the different incidences of ossified SSOs across population groups.(18) The difference in morphology of fan-shaped and band-shaped ossified STSLs, as observed in the present study, may be due to varying degrees of ossification extension into the STSL. Metabolic bone diseases and disorders of mineral metabolism, such as fibrodysplasia ossificans progressiva, have been suspected to cause ligament and tendon ossification.(19)
In the present study, two types of ossified STSL were observed – fan-shaped and band-shaped (
An ossified ITSL, which was also observed in the present study, can also result in SSN compression in the spinoglenoid notch; it is in the exact vicinity of the posterior portal and the Nevasier (supraspinatus) portal during shoulder arthroscopy.(20) An ossified ITSL could also cause confusion in surgeries that are performed around the shoulder area, as this entity is not widely described. Dynamic compression of the SSN by ossified ITSLs during glenohumeral range of motion in cadaveric shoulders has been reported by Plancher et al;(21) the authors concluded that dynamic compression by the spinoglenoid ligament during repetitive shoulder abductions is an important but often overlooked factor in posterior shoulder pain.(21) Thus, an ossified ITSL could be a cause of SSN compression in an osseous spinoglenoid foramen, during overhead and repetitive shoulder movements (hence, SSN compression of this nature may be more prevalent in sportspersons).
Bony tunnels were observed in two specimens in the present study. Bony tunnels may be a cause of scapular tunnel syndrome, as reported in Duparc et al’s study of 30 cadaveric shoulders in which supraspinatus fascia was the cause of tunnel syndrome.(1) The report concluded that in pathologic and posttraumatic conditions, the fascia may be retracted or thickened and SSN may be entrapped along its course in the supraspinatus fossa, between the suprascapular notch and spinoglenoid notch.(1)
In conclusion, variations in the morphological parameters of ossified ligaments might be directly related to SSN entrapment. While earlier observations of STSLs have been cadaveric with no precise osteological measurements to support their findings, the present study was an attempt to bridge these gaps while studying less investigated domains of ossified scapular ligaments. We reported data on the quantitative classification of ossified STSLs, as well as the dimensions of rarely documented cases of bony tunnel and ossified ITSL in the scapula. Such information is clinically relevant, especially in open and arthroscopic interventions for SSN decompression, and in suprascapular nerve blocks within the scapular region.