

Abstract
A 50-year-old Chinese man presented with abdominal pain associated with bloody mucoid stools, loss of appetite and weight loss. Contrast-enhanced computed tomography of the abdomen and pelvis revealed a colocolic intussusception secondary to a lipoma. The patient subsequently underwent a left hemicolectomy. Clinical and imaging findings of intussusception in adults are discussed in this article.
CASE PRESENTATION
A 50-year-old Chinese man who had no significant past medical history presented with a one-month history of bloody stools mixed with mucus. This was associated with suprapubic abdominal pain, loss of appetite and weight loss of 4 kg over the past month. He did not complain of haematemesis, chest tightness or giddiness.
Physical examination revealed mild suprapubic tenderness with no evidence of guarding or rebound tenderness. The bowel sounds were active and digital rectal examination showed soft brown stools within the rectum, with no melaena or mass felt. Supine abdominal radiography (
Fig. 1
Supine radiograph of the abdomen.
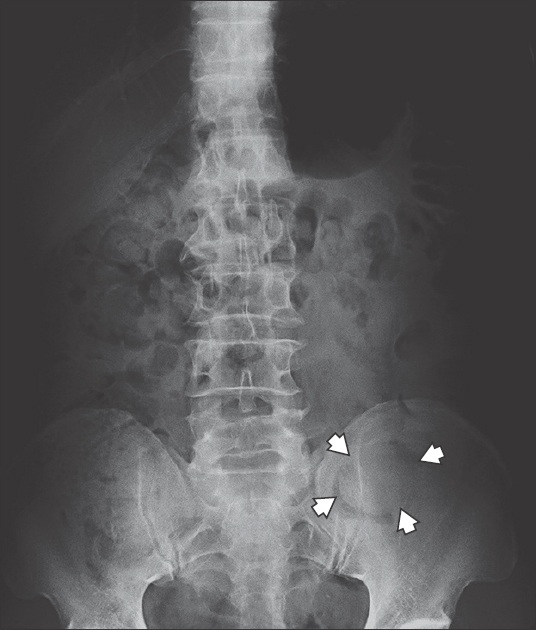
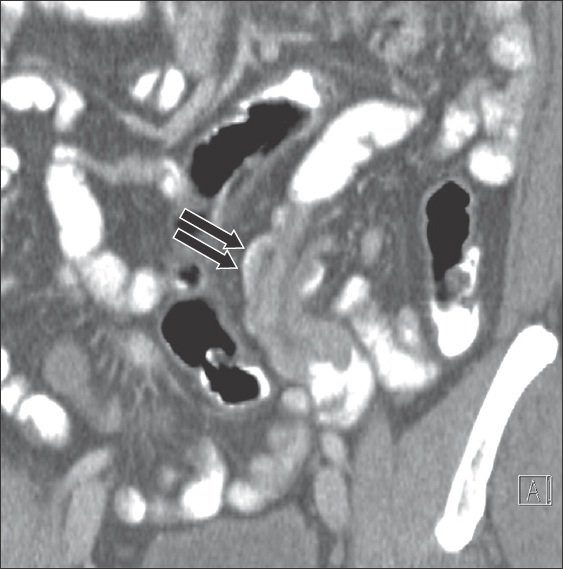
Fig. 2
(a & b) Axial and magnified; (c) coronal; and (d) sagittal CT images of the abdomen and pelvis in the portal venous phase.
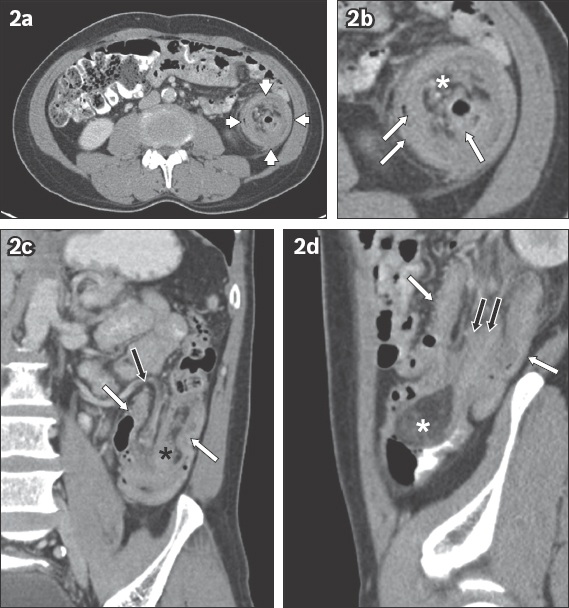
IMAGE INTERPRETATION
The supine abdominal radiograph (
DIAGNOSIS
Colocolic intussusception with a lipoma as the lead point.
CLINICAL COURSE
On-table sigmoidoscopy performed on the patient showed a polypoid whitish mass 30 cm from the anal verge, which was completely occluding the lumen. He subsequently underwent a laparotomy that showed no evidence of a colocolic intussusception. However, the distal segment of the sigmoid colon was noted to be oedematous and indurated. A hard, mobile mass was palpable within the descending colon, with no invasion of the surrounding structures. No lymphadenopathy, peritoneal disease or dilated small bowel loops were seen. A left hemicolectomy was then performed. Although there was no intussusception seen during surgery, the imaging findings were unequivocal for intussusception. It can be postulated that the prolapsed bowel spontaneously reduced shortly after the sigmoidoscopy was performed.
Gross pathological examination revealed a polypoid mass measuring 6.6 cm × 3.6 cm × 2.3 cm in the descending colon, with surface ulceration and haemorrhage. The segment of the colon distal to the mass was oedematous. Histological examination showed the mass within the descending colon to be a submucosal lipoma. There was no evidence of dysplasia or malignancy. The patient’s post-surgery recovery was uneventful, with no further complaints on follow-up.
DISCUSSION
Intussusception is a recognised but rare cause of intestinal obstruction in the adult population. Adult intussusception (AI) makes up 5% of all cases of intussusception and only 1%–5% of intestinal obstruction in adults.(1) This is in contrast to the paediatric population, in which the most common cause of intestinal obstruction in infants aged 6–36 months is intussusception.(2)
The condition is characterised by the invagination of a proximal loop of bowel (termed the intussusceptum) into a distal loop of bowel (known as the intussuscipiens), similar to how the parts of a collapsible telescope slide into one another. This gives rise to a ‘bowel-within-bowel’ appearance that can be recognised on imaging studies. The process of invagination pulls the mesenteric fat and vessels into the plane between the intussusceptum and intussuscipiens. This causes kinking of the vessels, resulting in vascular congestion, bowel ischaemia and perforation in severe scenarios.
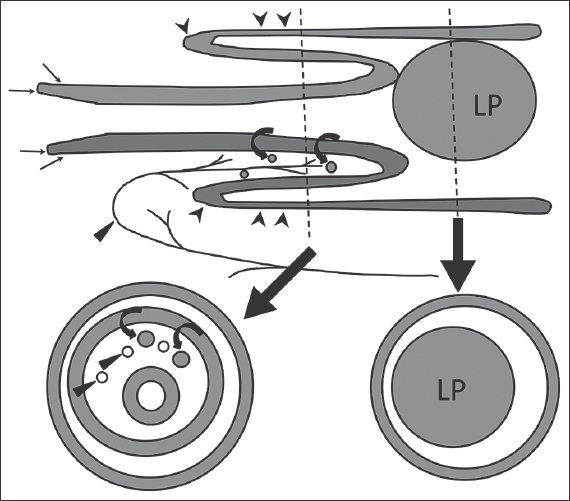
Fig. 3
Schematic diagram of an intussusception shows the telescoping of one segment of the bowel (intussusceptum, thin black arrows) into the adjacent segment (intussuscipiens, black arrowheads). Cross-sectional diagram of the mid-segment of the intussusception shows the classical target-like appearance with three layers of bowel. Note the dragging of the mesenteric vessels (indicated by black triangles) and hyperplastic lymph nodes (curved black arrows) along with the intussusceptum [adapted from Choi SH, et al].(3) LP: lead point
Patients with AI commonly present with nonspecific abdominal symptoms and features of intestinal obstruction that may have an acute, intermittent or chronic course. Only 9%–10% of adult patients present with the classic triad: acute colicky abdominal pain; passing of ‘currant jelly’ stool; and a palpable mass in the abdomen.(4) The location of AIs can be broadly divided into enteric and colonic. In a literature review conducted by Felix et al, out of 1,214 adult patients with colonic and small bowel intussusception, 55% occurred in the small bowel and 45% were colonic.(5) 70%–90% of AIs have an underlying lesion that acts as a lead point for telescoping to occur.(1) Lead points are thought to either alter the normal peristaltic movements of the bowel, or act as an intraluminal mass that is propelled in the antegrade direction by peristalsis, thereby pulling a segment of bowel along with it.
Numerous entities can act as a lead point, but a malignant tumour of the bowel is the cause for most concern. In Felix et al’s literature review, 48% of colonic intussusceptions (261/546) were found to be due to a malignant tumour; conversely, only 17% of all small bowel intussusceptions (116/668) were due to malignancy.(5) Given that a significant proportion of colonic intussusception in adults is due to malignancy, it is prudent for radiologists to be watchful for radiological features of malignancy, such as lymphadenopathy, irregular polypoid mass and liver metastases.
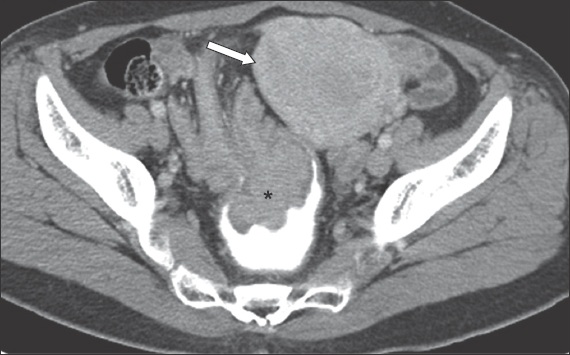
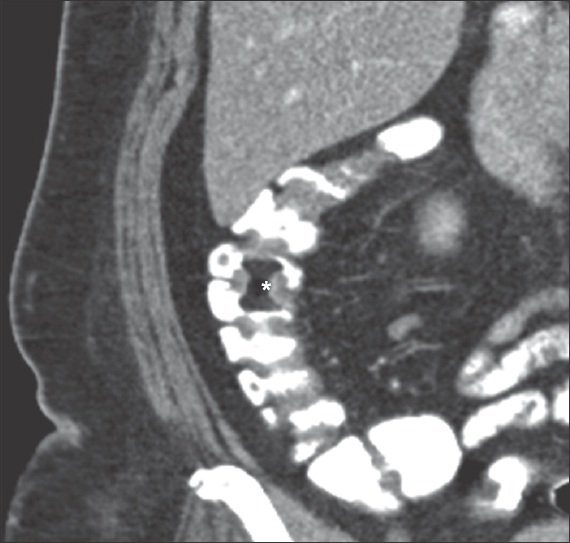
Fig. 4
Contrast-enhanced axial CT image of a female patient shows a colorectal intussusception with a polypoid soft-tissue mass (asterisk) at the apex of the intussusceptum. It is outlined by positive intraluminal contrast media in the rectum. The uterus is indicated by the white arrow.
Small bowel intussusception, a condition seen in both adult and paediatric populations, can be transient and self-limiting. In such cases of transient small bowel intussusception, no lead point can be identified; the length and diameter of the intussusception are shorter and smaller, respectively, and the proximal bowel loops are not dilated. Patients are usually asymptomatic, and telescoping of small bowel loops is occasionally seen when patients undergo CT or ultrasonography for an unrelated condition.(6,7)
Fig. 5
Contrast-enhanced oblique coronal CT of the abdomen performed in a patient who presented with weight loss and anaemia. A small bowel intussusception (black arrows) is seen in the left lower quadrant with no features of intestinal obstruction. No lead point is identified.
Although a significant proportion of AIs have a malignant tumour as a lead point, benign tumours such as lipomas can also be responsible, as shown in our case. Lipomas are the second most common benign tumour of the colon, with an incidence of up to 4% in autopsy series.(8) They are often discovered incidentally when a patient undergoes a radiological examination for an unrelated cause.
Fig. 6
Contrast-enhanced coronal CT image shows a lipoma (asterisk) within the ascending colon in a patient who was evaluated for an unrelated condition. The lipoma is outlined by positive contrast media within the ascending colon.
Lipomas are the most common benign tumour found in cases of large bowel AI.(9) From 2001 to 2011, 50 cases of AI induced by a lipoma were reported in the English literature, of which 23 cases were lipomas arising from the colon.(10) The imaging findings of another patient who presented to our institution with intussusception due to a lipoma are shown in
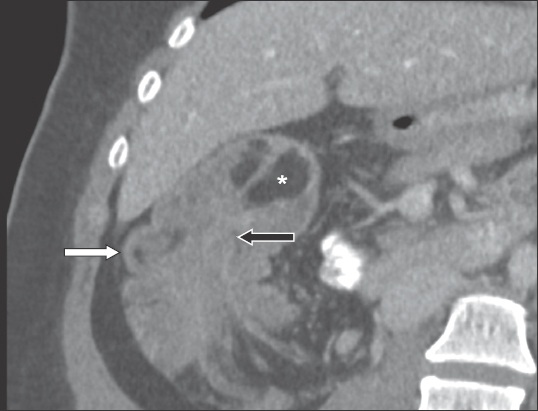
Fig. 7
Coronal CT image of the abdomen and pelvis in portal venous phase shows a lipoma (asterisk) at the apex of the intussusceptum (black arrow). The ascending colon (white arrow) is the intussuscipiens. Laparotomy showed a caecal-colic intussusception.
Radiology remains crucial in the diagnosis of intussusception. Plain radiography is helpful to exclude pneumoperitoneum, which would necessitate urgent surgical intervention. In some patients, the intussusceptum may be seen as a soft-tissue mass in the right upper quadrant, outlined by a crescent of gas within the colonic lumen (also known as the ‘meniscus sign’).
In recent years, multidetector CT of the abdomen and pelvis has increasingly become the imaging modality of choice for evaluating the adult patient suspected to have intussusception.(9) CT is able to diagnose intussusception by demonstrating a target-like mass with alternating layers of low-density mesenteric fat and soft-tissue density bowel walls. Enhancing mesenteric vessels are also seen within the mesenteric fat as it accompanies the intussusceptum. In addition, CT may be able to identify the lead point responsible for the intussusception, exclude other causes of abdominal pain or intestinal obstruction, and evaluate for complications such as perforation and bowel ischaemia. The accuracy of CT in diagnosing AI was shown to be 78% in one study.(1) In another study, the sensitivity of CT was > 85% for single- and multi-slice scanners.(11) The drawbacks of CT include the use of ionising radiation in acquiring images and the possibility of breathing artefacts in ill patients.
Ultrasonography is essential in the diagnosis of intussusception in children. The small body habitus of most children allows for the use of high-frequency transducers to produce images with good spatial resolution. The diagnosis relies on the recognition of the ‘bowel-within-bowel’ appearance on ultrasonography. The ‘target’ and ‘pseudokidney’ signs describe the appearance of the intussusception in the transverse and longitudinal planes, respectively. Ultrasonography has a high sensitivity for the diagnosis of intussusception in children (98%–100%).(12) It is also advantageous, as it does not utilise ionising radiation and allows for portable imaging if the patient is too ill to be transported to the radiology department. Despite these advantages, the accuracy of ultrasonography in the diagnosis of AI is low (50%).(13) This can be attributed to operator experience, the larger size of adult subjects, and the presence of bowel gas, which leads to poor transmission and difficulty in image interpretation.
Given that a large proportion of AIs have a lead point, which incidentally also has a relatively high incidence of malignancy, surgical resection is the recommended treatment, regardless of whether the intussusception is located in the colon or small bowel.(5,14) In contrast, most cases of intussusception in children do not have a lead point. As such, fluoroscopically-guided air-enema reduction is the recommended treatment. Surgical exploration is considered if there are multiple recurrences of intussusception despite successful air-enema reduction, failed air-enema reduction, or when there are signs of perforation, bowel gangrene or necrosis.(12)
SMJ-57-668.pdf