

Abstract
The role of the dispatch centre has increasingly become a focus of attention in cardiac arrest resuscitation. The dispatch centre is part of the first link in the chain of survival because without the initiation of early access, the rest of the chain is irrelevant. The influence of dispatch can also extend to the initiation of bystander cardiopulmonary resuscitation, early defibrillation and the rapid dispatch of emergency ambulances. The new International Liaison Committee on Resuscitation, the American Heart Association and, especially, the European Resuscitation Council 2015 guidelines have been increasing their emphasis on dispatch as the key to improving out-of-hospital cardiac arrest survival.
INTRODUCTION
Out-of-hospital cardiac arrest (OHCA) is inherently hard to survive. In Singapore, although the survival rate of witnessed cardiac arrests with a ventricular fibrillation origin has climbed from 2.5% (2001–2004) to 11.0% (2010–2012),(1) and overall cardiac arrest survival has increased from 1.6% to 3.2%, there is still room for improvement in many areas. In 2010–2012, bystander cardiopulmonary resuscitation (CPR) rates increased from 19.7% to 22.4% and public access defibrillation was attempted in 1.8% of cases, with 1% of the OHCA cases being defibrillated. Cardiac arrest is extremely time sensitive; without any intervention with CPR or defibrillation, survival drops at an average rate of 7%–10% per minute.(2) In 1985, Eisenberg et al first described the implementation of dispatcher-assisted CPR (DACPR) as a means of coaching untrained bystanders in King County, Washington, United States.(3) This seminal work showed that bystander CPR increased from 45% to 56% after the implementation of the protocol. Remarkably, the unassisted bystander CPR rate in King County then was already notably high, at 45%.
KEY ROLE OF DISPATCH IN THE CHAIN OF SURVIVAL
‘Early access’, the first link in the chain of survival, denotes the recognition of cardiac arrest as well as the rapid activation of emergency medical services (EMS).(4) In 2015, both the American Heart Association (AHA) and European Resuscitation Council (ERC) guidelines emphasised the importance of dispatch in improving OHCA survival. The modern dispatch centre’s role extends beyond activating EMS, a complex process by itself. The ERC guidelines highlight the significant role that dispatchers play in guiding the bystander to perform CPR, deploying public access automated external defibrillators (AEDs), and rapidly and accurately guiding the EMS to the site of the incident. It is increasingly evident that the dispatcher exerts a high level of influence over the first three links in the chain of survival. Scientific evidence has also led to strong recommendations for identifying agonal breathing over the phone as an early indicator of OHCA, coaching/coaxing bystanders to initiate hands-only CPR effectively and increasing the use of public access defibrillation to raise survival outcomes.(4)
Diagnosing cardiac arrest over the telephone
The best practice today for recognising OHCA over the telephone is based on asking the caller two questions: “Is the patient unconscious?” and “Is the patient breathing abnormally or not breathing?” The evidence for this has been gathered from 27 observational studies involving more than 17,000 patients and shown to have a sensitivity of 38.0%–96.9% and a specificity exceeding 97%. If the answer is ‘yes’ to both questions, cardiac arrest is presumed, and a standardised script of just-in-time instructions over the telephone is used to maximise the likelihood of helping the caller to perform the activities needed to start chest compression-only CPR in adults or CPR with ventilations in children or those suspected of having respiratory arrest.(5)
Can untrained persons be coached to perform CPR during a cardiac arrest?
In 1989, Kellerman et al(6) compared CPR performed on manikins by three groups of volunteers: one group was untrained and given telephone instructions; one group had only CPR training; and the last group was trained in CPR and given telephone instructions. The study showed that telephone instructions can guide even untrained people to perform correct chest compressions with better consistency in rate and depth over five minutes compared to people with CPR training. As expected, those with both CPR training and telephone coaching had the best outcomes. In 1989, the protocols included the teaching of ventilation instructions, which was highlighted to be inferior to prior CPR training.
Should dispatchers give instructions on full or hands-only CPR?
Both the AHA and ERC 2015 guidelines(4,7) unequivocally recommend the coaching of hands-only CPR to untrained responders. Based on current evidence, a meta-analysis of three randomised controlled trials comparing chest compression-only CPR against chest compression with ventilation instructions showed an absolute increase in survival in the chest compression-only group by 2.4%, but currently there is no evidence that DACPR instructions lead to improved neurological survival.
Mouth-to-mouth ventilation with chest compression continues to be the standard for CPR training; however, in the context of DACPR instructions, it has been shown that it is difficult to teach mouth-to-mouth ventilation with chest compressions in a short amount of time.(8) Another prospective trial found that laypersons with limited training take an average of 16 seconds to provide two ventilations. Furthermore, giving mouth-to-mouth ventilation has been shown to be a clear barrier to initiating CPR among laypersons and healthcare workers.(9-11) Hence, the giving of ventilation instructions is recommended to be limited to children, drowning victims or adults with a suspected respiratory cause of cardiac arrest.
Recognising agonal breathing
Agonal respiration is a brainstem reflex and a respiratory pattern often seen in the early stage of cardiac arrest.(12) It is sometimes described as a dying man’s breath. It has been described as sighing, gasping, choking or snorting, and is slow or intermittent in rate.
Agonal breathing was first characterised by Clark et al in 1992 to be present in 40% of 445 cases of OHCA; it was notably more frequent in witnessed arrest (55%) compared to unwitnessed arrest (16%), occurred more often in ventricular fibrillation (56%) compared to non-ventricular fibrillation (34%), and found to be associated with higher survival to discharge (27%) compared to those who did not have agonal breathing (9%).(13) Further studies over the years have confirmed these findings, and training of dispatchers to specifically recognise agonal breathing became a key recommendation in the ERC and AHA 2015 guidelines(4,7) for the implementation of a successful DACPR programme.
However, agonal breathing is also postulated to pose a barrier to the initiation of CPR.(14,15) In one review of 404 audio recordings, signs of life was reported as the most common reason (51%) for not offering DACPR instructions.
Should hands-only CPR be started presumptively?
Identifying cardiac arrest over the telephone is a challenging activity, given that the dispatcher has no visual cues and a limited amount of time to interrogate the caller. A further challenge is that the caller may interpret the questions and instructions in a wide variety of ways, potentially leading to overdiagnosis of cardiac arrest (false positive) and chest compression being performed on a person who is not in cardiac arrest.
White et al, in a prospective study,(16) specifically addressed the above question by collecting follow-up data on the outcomes of 1,700 patients who were given DACPR. 45% of the patients (762/1,700) were not in arrest. However, bystander chest compression was initiated in 18% of the cases (313/1,700); 247 of these cases were traced and followed up – 12% (29/247) complained of chest discomfort, 2% (5/247) sustained fractures, but none sustained any visceral organ damage. The study estimated that DACPR enabled a 25% increase in bystander CPR in the community, with an 18% false positive rate (313/1,700) and a 0.3% injury rate (5/1,700). Therefore, the study concluded that the benefits of initiating chest compressions in a suspected OHCA case far outweigh any potential harm.
Can untrained persons use a public access defibrillator?
The ERC 2015 guidelines support the use of AEDs by laypersons with no or minimal AED training.(7,17) Guidance by a dispatcher can potentially increase the success rates of delivering a public access AED to the scene of a cardiac arrest, but limited scientific data is available to quantify the effects of the role played by the dispatcher. In the Public Access Defibrillator Trial, in which 1,716 AEDs were deployed over 26,389 exposure months, no inappropriate shocks were given and no serious accidental injuries of rescuers occurred (one reported a muscle pull, four experienced significant emotional distress and two reported pressure from their employer to participate).
What role does the dispatcher play in raising AED utilisation?
There are few countries around the world where AED registration is mandated. Of note, Taiwan and Korea both have AED-related legislation, mandating the installation of AEDs in certain public places, as well as regular mandatory reporting of the AED locations to the national registry.
In most places, AED locations are mapped through community projects or other means. In Singapore, there is currently no legislation or regulation mandating the installation or maintenance of AEDs in public places, and public access AEDs are mapped through a community partnership between the Ministry of Health (MOH), Singapore Civil Defence Force (SCDF) and Singapore Heart Foundation (SHF). The locations of the AEDs are recorded and available to the public (
Dispatchers play an important role in improving early defibrillation. A recent paper from Denmark(18) decribed how a volunteer organisation, TrygFonden, worked closely with the Emergency Medical Dispatch Centre to establish a sophisticated online network to register AED locations and their accessible hours. The network is integrated with the dispatch centre to enable the caller to be directed to the nearest AED (within 100 m) or to call the AED owner to deliver it to the scene of a cardiac arrest. The network then inactivates the AED that is in use until it is restored and validated by the owner for operational use by the dispatch centre.
Fig. 1
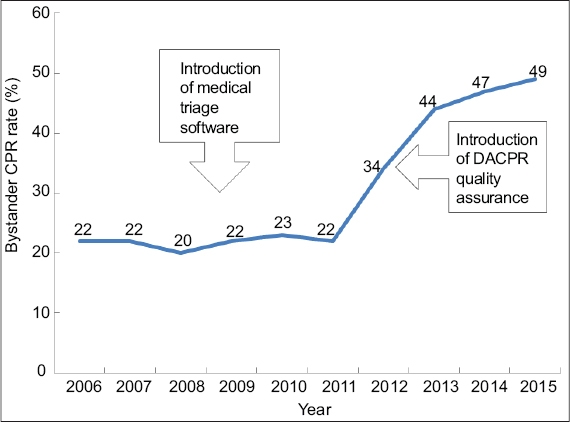
Bystander cardiopulmonary resuscitation (CPR) data from the Singapore Civil Defence Force ambulance records (2006–2015).
SOCIAL MEDIA, CROWDSOURCING AND TECHNOLOGY IN FIRST RESPONSE
Owing to the ubiquitous ownership of smartphones, especially in Singapore, social media and crowdsourcing are now increasingly viable tools that dispatch centres can utilise to enhance the success of the chain of survival.(19) Mobile devices have the ability to provide highly accurate location data, visual communication, navigation guidance, and basic vital sign and health information through common wearable devices.
Mobile applications can also be used to teach basic awareness and impart knowledge on recognition of cardiac arrest, chest compression and AED usage through ‘gamification’, a process of teaching serious subjects by making the experience game-like.(20) Gamification is also increasingly used to induce behavioural changes such as encouraging a healthy lifestyle or volunteerism, and even imparting new skills.
In Singapore, the SCDF ‘myResponder’ app, launched in April 2015, is one such social media application that allows CPR-trained persons to register themselves to receive alerts from SCDF’s 995 dispatch centre if a potential cardiac arrest case occurs within 400 m of their vicinity.(21) It also contains the locations of public access AEDs that are registered and verified by SHF, so that the responder can retrieve an available AED and bring it to the scene of a cardiac arrest for early defibrillation. The app has been credited with summoning a trained volunteer to perform CPR on a cardiac arrest victim, leading to survival to discharge with good neurological outcome.(22)
This idea has been further expanded through a partnership with Temasek Foundation Cares and SMRT Taxis to equip with AEDs 100 CPR-trained taxi drivers, who can respond within a driving radius of 1.5 km while on duty, hence increasing the chances of bringing an AED to the scene of a cardiac arrest.
DISPATCHER-ASSISTED CPR IN SINGAPORE
In Singapore, most emergency calls are taken by firefighters. In 2009, medical triaging software was implemented to aid dispatchers in providing pre-arrival instructions within a computer-aided dispatching system, but the potential of it was fully realised only in mid-2012 with the implementation of a telephone CPR quality assurance programme. This was achieved through interviews, surveys and comprehensive reviews of audiotapes for the collection of quantitative and qualitative data to initiate a review of call-taking instructions and for the purpose of setting up an OHCA call-taking research registry.(23)
These efforts were further complemented by the following: DACPR training workshops organised for all SCDF Call Centre dispatchers in 2012; secondment of four Singapore General Hospital nurses to the centre to conduct audiotape reviews; and in-house dispatcher medical training since 2013. This has contributed to the increase in bystander CPR rates in Singapore, from 22% in 2011 to 49% in 2015.
CONCLUSION
The fastest ambulance in the world cannot be faster than the bystander at a patient’s side. DACPR is a proven key enabler of the first three links within the chain of survival, and in recent years, its importance as a very low cost, but highly effective, means to raise bystander CPR rates in an environment with limited resources has started to gain recognition. DACPR alone cannot be the solution to cardiac arrest, because formal CPR training is still superior to just-in-time training when both are guided by a dispatcher. However, in the absence of a trained person, any CPR done early is better than waiting for the ambulance crew to arrive to perform CPR.(24)