

Abstract
Paediatric liver transplantation has come a long way since its acceptance as a treatment option for children with end-stage liver disease. From 1990 to 2020, a total of 434 liver transplants were performed in National University Hospital, Singapore, out of which 143 were performed in children. The majority of the liver grafts were from living donors, mainly the parents. Our long-term survival rates are comparable to those of major transplant centres worldwide. These patients usually have a productive and good quality of life.
INTRODUCTION
Liver transplantation (LT) has come a long way since its acceptance as a treatment option for patients with end-stage liver disease. The outcome of LT for paediatric recipients is no longer aimed at just survival but other measures such as good catch-up growth and quality of life. In fact, many studies have shown that the health quality of LT recipients significantly improves within six months after a successful transplant. Paediatric liver transplantation accounts for about 10% of the total number of LTs performed annually. Improvement in patient selection, pre- and postoperative care, surgical techniques, organ preservation as well as immunosuppression have resulted in excellent post-transplant survival and quality of life.
The first LT in Singapore was performed in 1990 in a patient with autoimmune hepatitis.(1) Since then, over 434 LTs have been performed in the National University Hospital (NUH), 143 of which have been in children. The paediatric transplant programme is based at the NUH. It comprises a multidisciplinary team, including transplant co-ordinators, transplant surgeons (adult and paediatric), paediatric gastroenterologists, paediatricians from various subspecialties, dieticians, nurses, pathologists, social workers, physiotherapists, radiologists and adult physicians (who assess the adult living donors). The programme also receives invaluable support from doctors in both public and private sectors. Prof Phua Kong Boo and Dr Ooi Boo Chye from KK Women’s and Children’s Hospital were the first visiting paediatric consultants to the programme.
INDICATIONS FOR LIVER TRANSPLANT
LT is indicated when the risk of mortality from one’s native liver disease outweighs the risk of transplant. In general, a child should live with his/her own liver for as long as possible. Although LT is lifesaving, it carries the risks of surgery as well as the need for life-long immunosuppression. Children with chronic liver disease should be considered for LT in cases of faltering of growth, deteriorating synthetic function, progressive jaundice and intractable ascites. Severe intractable pruritus in the absence of decompensated liver disease is a relative indication. Although rare, fulminant liver failure would be an urgent reason for LT. While many of the cases of acute fulminant liver failure are idiopathic, some of the identifiable causes include viruses, drugs (medications) and metabolic disease. Contraindications to transplantation include uncontrolled systemic infection, unresectable malignancy outside the liver, genetic or metabolic conditions not treatable by liver transplant alone and irreversible severe neurologic injury.
LT is a labour-intensive and expensive procedure, both in term of finances and resources. A strong family support is required in order to ensure that the child adheres to the medications and treatment plans. It is vital that the child’s parents and caregivers are able to provide the care and close supervision after transplant. At the same time, the members of the LT team (nurse specialist, medical social worker) should also be able to provide the family with the necessary education, counselling and psychosocial support.
PATIENT CHARACTERISTICS
Between 1991 and 2020, 143 LTs were performed in 135 children. Eight of these patients underwent a second LT because the first graft had failed. The aetiologies for LT in these 135 children are shown in
Table I
Indications for paediatric liver transplant in National University Hospital (n = 135).
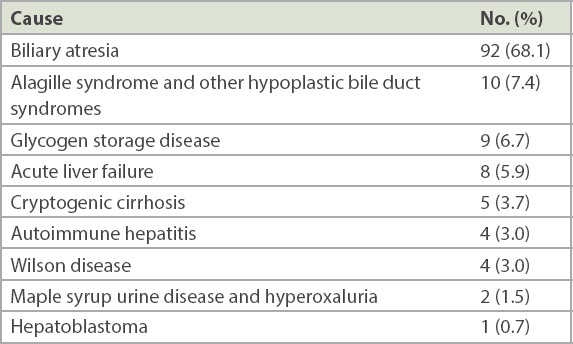
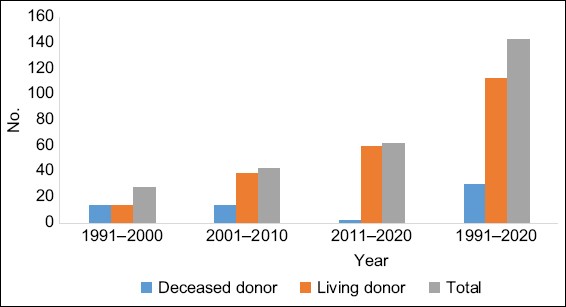
Fig. 1
Graph shows the number and type of liver transplants performed in each decade.
SURVIVAL
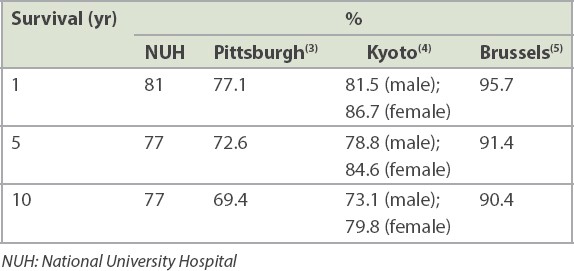
Paediatric LT recipients have shown excellent post-transplant survival outcomes.
Table II
Comparison of survival rates after liver transplantation.
COMPLICATIONS
Several complications can occur following LT. Surgical-related issues(6) include those associated with biliary and vascular problems. These range in severity from requirement of minimal intervention to the need for re-transplant. Perihepatic fluid collections suggestive of biliary leak are not uncommon. Some of them resolve spontaneously, whereas others may require percutaneous drainage or open laparotomy. Isolated biliary strictures are treated by biliary stenting, while those with multiple strictures following secondary ischaemia may require re-transplant.
Vascular complications include hepatic vein thrombosis or stricture, hepatic artery thrombosis and portal vein thrombosis. Early hepatic and portal vein thrombosis are managed by surgical thrombectomy and re-do anastomosis. Hepatic vein thrombosis can be overcome by balloon dilation under radiology guidance by our interventional radiologists. We had encountered a patient with an anastomotic stricture of the hepatic vein, which underwent multiple balloon dilations.
Infections remain an important issue in LT, particularly opportunistic infections in the long term. Bacterial infections, with the sites of infection being intra-abdominal or line-related, would be the main concern in the immediate postoperative period. Paediatric recipients are routinely administered broad-spectrum antibiotics in the immediate postoperative period, and these are discontinued once all invasive lines and tubes are removed, or adjusted according to bacterial cultures if there is evidence of systemic infection. Patients exposed to broad-spectrum antibiotics prior to transplant or those in whom acute liver failure was the reason for transplant would have a relatively low threshold for antifungal therapy.
Of all the opportunistic infections, Epstein-Barr virus-related post-transplant lymphoproliferative disease (PTLD) is of particular concern in children. The overall incidence of PTLD in our paediatric transplant recipients is about 16%.(7) The risk of PTLD is higher in children aged < 2 years at transplant, those who develop primary cytomegalovirus (CMV) infection after transplant and those who experience acute cellular rejection. There appears to be synergism between CMV naivety and acute cellular rejection on the risk of developing PTLD.
Acute cellular rejection (ACR) is not uncommon and, in some instances, is believed to be harmless if it occurs within the first four to six weeks after transplant. Most of the time, ACR can be reversed by intensifying immunosuppression therapy. Although some patients show more resistant forms of rejection, the general requirement for immunosuppression in LT recipients is less than that required for recipients of other solid organ transplants such as the kidney or the heart. Theoretically, ACR can occur any time after LT. Later occurrence is associated with a greater risk of non-adherence. Graft loss from non-adherence has been reported, mostly among adolescent patients.
QUALITY OF LIFE
In terms of quality of life, our LT recipients have acceptable pedQoL score compared with the normal population. They also show good physical and social functioning scores.(8) As shown in
CONCLUSION
Paediatric LT in Singapore has come a long way. Biliary atresia accounted for about two-thirds of our cohort of 135 patients. The one-, five- and ten-year survival rates are good and comparable to those of other major centres worldwide. Several concerns related to LT have been highlighted. Shortage of deceased donor organs resulted in the emergence of living donors as the main mode of LT among children in Singapore. Although LT is a labour- and resource-intensive procedure, careful selection of patients along with good patient and family support before and after transplant would ensure successful LT and the best patient outcomes.