Abstract
Inhalation injury is a serious consequence of a fire or an explosion, with potential airway compromise and respiratory complications. We present a case series of five patients with inhalational burns who presented to Singapore General Hospital and discuss our approach to their early management, including early evaluation and planning for the upper and lower airway, coexisting cutaneous burns, and monitoring their ICU (intensive care unit) severity of illness, sepsis and acute respiratory distress syndrome. All five patients suffered various grades of inhalation injury. The patients were initially assessed by nasolaryngoscopy, and three patients were prophylactically intubated before being sent to the emergency operating theatre for definitive airway and burns management with fibreoptic bronchoscopy. All patients were successfully extubated and discharged stable. Various complications can arise as a result of an inhalation injury. Based on our cases and literature review, we propose a standardised workflow for patients with inhalation injury.
INTRODUCTION
Inhalation injuries, which may occur as a result of a fire or an explosion in an enclosed space, can be associated with cutaneous facial burns and coexisting trauma. Specific complications include thermal injury and swelling of the upper and lower airway, bronchospasm, bronchial obstruction with carbonaceous sputum plugs, pneumonia, acute respiratory distress syndrome (ARDS), carbon monoxide toxicity and cyanide toxicity, as well as the complications of coexisting cutaneous burns and trauma, if present. Hence, the initial triage and approach to patient management focuses on these areas. We present a case series of five patients with inhalational burns in 2017 (
Table I
Patient characteristics.
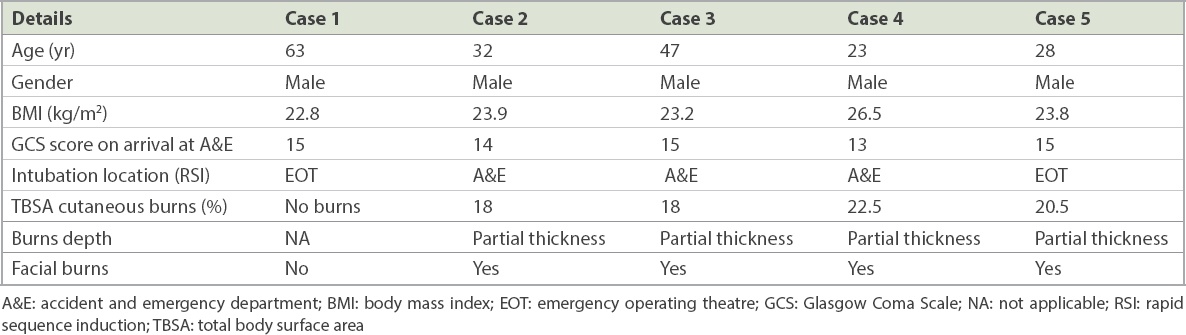
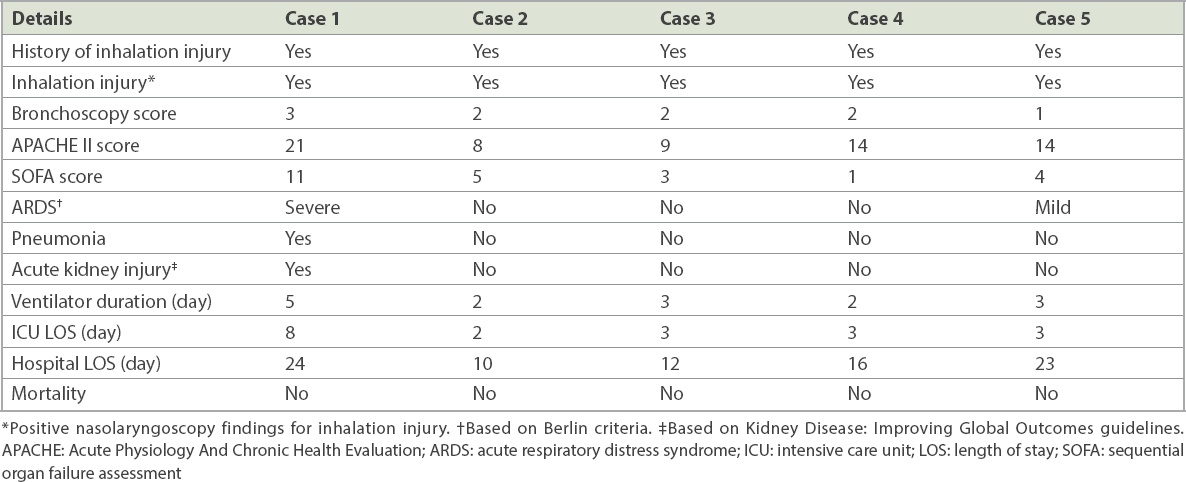
Table II
Patient outcomes.
This retrospective review of the burns database was approved by the SingHealth Centralised Institutional Review Board. Written informed consent was obtained from the patients for publication of this case report and the accompanying images. Data was collected from the internal network database of Singapore General Hospital, Singapore.
CASE SERIES
Patient 1
A 63-year-old man had fallen asleep when his candle dropped on the living room floor and set fire to the windowsill. He suffered an inhalation injury but no cutaneous burns. At presentation to the accident and emergency department (A&E), the patient was well with no stridor or change of voice. On bedside nasoendoscopy, he was found to have minimal soot in the anterior and posterior nasal space, with some soot in the glottis, base of the tongue, posterior cricoid and subglottic region. The larynx was not swollen.
Although chest radiography was clear on admission, the patient desaturated 24 hours after presentation. Wheeze and transmitted sounds were heard on auscultation. Subsequent chest radiography demonstrated bilateral lower lobe collapse with increased pulmonary congestion and consolidation, suggestive of pneumonia. Arterial blood gas showed Type 1 respiratory failure and metabolic acidosis. The patient was transferred emergently to the emergency operating theatre (EOT) for rapid sequence induction, endotracheal intubation and initiation of mechanical ventilation, and subsequently transferred to the BICU. Bronchoscopy showed a significant amount of thick mucous plugging, leading to pneumonia. In view of the thick mucous plugging, this was considered a Grade 3 inhalation injury based on the Endorf and Gamelli classification.
At the BICU, regular aggressive suctioning was done and bronchoalveolar lavage was performed. Daily arterial blood gas was monitored and serial chest radiographs were obtained. Intravenous piperacillin-tazobactam was given for pneumonia and intravenous vancomycin for coagulase-negative staphylococci on blood cultures. The patient was ventilated for five days and remained in the BICU for eight days. The pneumonia resolved while he was in the BICU, as shown by serial chest radiography. The patient was stable throughout his stay in the BICU and remained so until discharge.
Patient 2
A 32-year-old man was in a parking lot trying to jump-start a car battery when the engine exploded. He suffered 18% total body surface area (TBSA) burns as well as inhalation injury. At initial presentation at the A&E, the patient was alert but disorientated and moaning in pain. He was in an altered mental state with a Glasgow Coma Scale (GCS) score of 14/15. Bedside nasoendoscopy showed that the upper respiratory tract was swollen and the vocal cords mobile but slightly oedematous. No carbonaceous sputum was observed in the airways. The patient was intubated prophylactically at the A&E and sent to the EOT for a burns scrubdown and Biobrane™ dressing (Smith & Nephew, Singapore) application. Bronchoscopy was performed prior to surgery. The lower airway was normal with no swelling or particulate matter; however, erythema was present throughout. There was upper airway swelling. Grade 2 inhalation injury was identified.
In the BICU, the patient remained stable. Arterial blood gas was consistent with his condition and vitals were non-significant. The patient remained stable throughout his stay.
Patient 3
The patient, a 47-year-old taxi driver, had stepped out of his taxi when the car engine exploded. A second explosion caused the injury. He had 18% TBSA burns and inhalation injury. At initial presentation, the patient was alert, orientated and spoke clearly. There was no hoarseness of voice or stridor, and oedematous upper airway was seen on nasoendoscopy. There was no soot.
The patient was intubated prophylactically in the A&E in view of the laryngoscopy findings, although he was clinically stable. He was subsequently sent to the EOT for a burns scrubdown and Biobrane dressing application. Bronchoscopy was performed at the end of the operation. There was erythema, friable mucosa and bronchorrhoea but no significant carbonaceous plugs. However, the patient had mucosal oedema in the trachea and the main airways, with complete occlusion of the right middle lobe of the lung and significant intrabronchial haemorrhage, especially in the left lower lobe. This was classified as a Grade 2 inhalation injury.
The patient was noted to have some blood-stained aspirates postoperatively in the BICU. Oesophagogastroduodenoscopy showed mild non-erosive gastritis. He remained stable in the BICU otherwise and was successfully extubated.
Patient 4
A 23-year-old man was working in the engine room on a cargo ship when the main engine exploded and set the room on fire. He suffered 22.5% TBSA cutaneous burns and inhalation injury. At the time of presentation, the patient was able to obey commands and open his eyes spontaneously. However, he was not able to answer any questions and could only mumble, with a GCS score of 13/15. No hoarseness of voice or stridor was heard. Nasoendoscopy showed soot in the nasal aperture and erythema throughout the airway but no oedema.
In view of the potential for worsening airway oedema, the patient was prophylactically intubated in the A&E by direct laryngoscopy even though he was able to speak. He was transferred to the operating room urgently for a burns scrubdown and Biobrane dressing application. Fibreoptic bronchoscopy at the end of the procedure identified a Grade 2 inhalation injury with a moderate amount of erythema at the carina and the left main bronchus, and mild erythema and bronchorrhoea in the right main bronchus. Distal to the main bronchi bilaterally, the lower bronchial tree was free from erythema or carbonaceous deposits. Bronchoalveolar lavage was performed with 20 mL normal saline. The patient was transferred to the BICU and was sedated and ventilated following the procedure. He remained stable in the BICU.
Patient 5
A 28-year-old man was involved in the same incident as Patient 4, an engine room explosion aboard a cargo ship. He suffered 20.5% TBSA burns and inhalation injury. On initial presentation at the A&E, nasoendoscopy was performed. There was no soot, but mild erythema and oedema was present along the upper airway.
The patient was transferred emergently to the EOT to undergo a burns scrubdown and Biobrane dressing application. Fibreoptic bronchoscopy at the end of the procedure revealed a Grade 1 inhalation injury with patchy areas of erythematous lower airway mucosa. There were minimal carbonaceous deposits and some bronchorrhoea. Bronchoalveolar lavage with 40 mL normal saline was performed. The patient was again taken to the operating theatre two days after Biobrane dressing application for wound inspection and skin grafting for his deep dermal burns. He was initially agitated and required additional sedation but otherwise remained stable in the BICU.
DISCUSSION
We herein discuss the grading of the severity of inhalation injury, based on clinical history, examination findings, and upper and lower airway endoscopy findings. In addition, we discuss our approach to airway management and extubation assessment based on a review of the existing literature and our case series.
Initial evaluation of a patient presenting with a history of inhalation injury includes the standard Advanced Trauma Life Support (ATLS) approach.(1) This includes a history of the mechanism of injury, alerts, allergies and comorbidities, and a complete primary and secondary survey. Immediate assessment includes evaluation of conscious level and vital signs, airway with cervical spine stabilisation, breathing, circulation, and coexisting whole body burns and trauma.
Inhalation injury is typically associated with burns to the face, neck and chest, as well as a large percentage of TBSA burned. However, it may occur even in the absence of cutaneous burns. A history of a fire or explosion within a closed space, or direct injury to the face with steam, chemicals or fire, suggest a high likelihood of inhalation injury. The presence of carbonaceous debris in the mouth or nose and singeing of the nasal hairs are particularly suggestive of inhalation injury. Other clinical features may include facial or upper airway swelling, hoarse voice, drooling of saliva, dysphagia and stridor.(2)
Lower airway inflammation may lead to ARDS with non-cardiogenic pulmonary oedema related to inflammatory capillary leak, as well as bronchospasm, bronchorrhoea and impaired sputum clearance. The precipitation of carbonaceous soot particles in the lower tracheobronchial tree predisposes one to bronchial obstruction, lobar collapse and pneumonia. Other possible respiratory complications include carbon monoxide or cyanide toxicity, pneumothorax from blast injury, pulmonary aspiration related to reduced conscious level, chest wall restriction from circumferential burns around the thorax, and atelectasis related to abdominal distension.(3)
The immediate aims of management are summarised as follows:(4,5)
Administer high-flow face mask oxygen via a non-rebreathing face mask to all patients in view of the risk of carbon monoxide toxicity.
Complete ATLS primary survey, then the secondary survey when the primary survey has been completed, vital signs are normalising and resuscitation efforts have been established.
Perform upper airway fibreoptic nasolaryngoscopy under local anaesthesia to evaluate for: carbonaceous debris in the pharynx or larynx; and erythema or swelling of the pharynx, aryepiglottic folds and vocal cords.
Limit intravenous fluid therapy prior to definitive airway management in view of the risk of airway swelling and ARDS.
Transfer the patient emergently to the operating room for definitive airway management and lung-protective ventilation; diagnostic fibreoptic bronchoscopy to confirm the diagnosis of lower airway inhalation injury, with bronchoalveolar lavage if needed to clear any obstructing carbonaceous plugs; and damage control surgery (escharotomy, < 5% excision and debridement of necrotic areas, and Biobrane application).
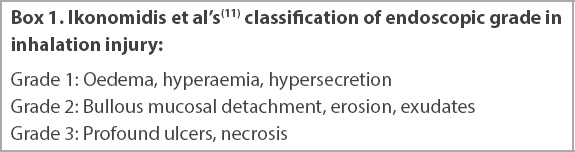
Several studies have identified factors associated with the need for early endotracheal intubation.(6-8) These include soot in the oral cavity; facial and neck burns; high TBSA of cutaneous burns > 27%; use of accessory respiratory muscles; elevated carboxyhaemoglobin (COHb) levels; and fibreoptic laryngoscopy findings of oedema, erythema or carbonaceous deposits on the true or false vocal cords. Importantly, features such as stridor, hoarse voice, drooling, dysphagia and singed nasal hair do not appear to be predictive of the need for early intubation, whereas fibreoptic laryngoscopy has emerged as a useful triage tool, with a high positive and negative predictive value.(9) Goh et al(10) described a modified triage system used in 22 patients presenting to the A&E following a smoke inhalation mass casualty incident. Clinical history, symptoms, signs and respiratory risk factors such as asthma were used for preliminary screening. Patients with risk factors for inhalation injury underwent fibreoptic laryngoscopy, chest radiography and arterial blood sampling for analysis of arterial blood gases and COHb levels. Patients with upper airway erythema or elevated COHb levels were admitted to hospital, whereas all other patients could be discharged home. Ikonomidis et al(11) conducted a prospective observational study in 100 patients with inhalation injury, in whom an endoscopic airway assessment was performed in the first few hours. An upper and lower airway endoscopy score was described, and lesions were classified as confined to the upper airway or with tracheobronchial extension. This is summarised in
However, while upper airway fibreoptic laryngoscopy is well tolerated and highly predictive of the need for intubation, it may be dangerous to attempt lower airway bronchoscopy in an unintubated spontaneously breathing patient with inhalation injury in the A&E, as required in the Ikonomidis classification system. In addition, lower airway bronchoscopy has a different purpose from upper airway laryngoscopy in inhalation injury. Whereas upper airway laryngoscopy is useful to predict the need for intubation, lower airway bronchoscopy is mainly useful in predicting the duration of mechanical ventilation, extubation planning, sputum clearance strategy and diagnosis of pneumonia.
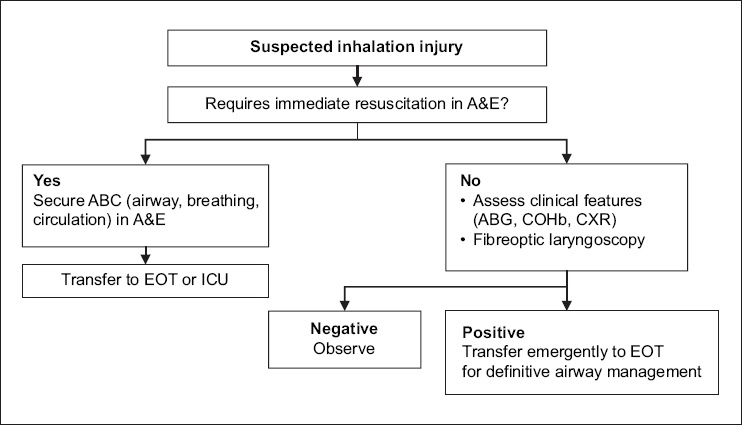
In our practice, we adopted a simple binary (yes/no) classification of upper airway laryngoscopy findings similar to that used by Muehlberger et al(9) and Goh et al,(10) compared with the more detailed classification proposed by Ikonomidis et al.(11) Hence, a stable patient with suspected inhalation injury receives an upper airway fibreoptic laryngoscopy, chest radiography, and arterial blood sampling for arterial blood gases and CoHb levels in the A&E, in addition to a standard clinical assessment. If any of these investigations or clinical features is abnormal, the patient is immediately transferred to the operating theatre for definitive airway management (
Fig. 1
Flowchart shows our institution’s protocol on intubating a patient with suspected inhalation injury. A&E: accident and emergency department; ABG: arterial blood gas; COHb: carboxyhaemoglobin; CXR: chest radiography; EOT: emergency operating theatre; ICU: intensive care unit
In the presence of inhalation injury, further airway swelling is likely once intravenous fluid resuscitation has begun, hence it is essential that the upper airway is secured and ventilation controlled urgently even if the patient has no respiratory failure and is fully conscious at the time of presentation. In patients presenting to the A&E in severe shock, endotracheal intubation may be required as part of initial resuscitation, particularly in the context of a reduced consciousness level, impending cardiorespiratory arrest, refractory hypoxaemia or refractory hypotension. Such patients may be too unstable to transfer to the operating room without first securing the airway. Coexisting cyanide toxicity, shock, and hypoxic or traumatic brain injury should be suspected in such cases. However, in most cases, patients with the following indications are stable enough to be transferred emergently for a planned endotracheal intubation in the operating room:(12,13) positive upper airway nasolaryngoscopy and planned fibreoptic bronchoscopy; reduced consciousness level; respiratory failure; stridor; facial or neck burns, singed nasal hair, or soot around the nares or mouth; facial or oropharyngeal swelling; inhalation injury; circumferential chest burns restricting breathing; planned damage control surgery for burns debridement and coverage; and planned interhospital transfers to specialist burns centres.
All patients with inhalation injury, burns, trauma or any critical illness are anticipated to have a risk of difficult endotracheal intubation, difficult mask ventilation, pulmonary aspiration and cervical spine instability if there is coexisting trauma. In addition, respiratory and haemodynamic instability is anticipated following intubation and initiation of mechanical ventilation. In inhalation injury, the airway is dynamically evolving with increasing facial and airway swelling over time, particularly after the initiation of intravenous fluid therapy. This makes failed intubation, potentially resulting in hypoxic cardiac arrest and/or hypoxic ischaemic encephalopathy, more likely with any delay. Hence, early transfer to the EOT for definitive airway management is considered a time-critical intervention in patients with inhalation injury, as specialised airway equipment and staff, including anaesthesiologists and surgeons, would be available to perform a surgical airway or local anaesthetic tracheostomy if required.
Options for securing the airway include maintenance of spontaneous breathing with an awake intubation technique under upper airway local anaesthesia in compliant patients, or a rapid sequence induction (RSI) technique with general anaesthesia and abolishment of spontaneous breathing in non-compliant patients. If an RSI technique is chosen, it is important to note that suxamethonium is contraindicated after the first 24 hours following acute burns, in view of the risk of hyperkalaemia.(12) This may be relevant in patients who present late to the A&E, or are transferred from regional centres, several hours after sustaining their injury. Routine preparation for intubation typically includes dual oxygen administration with nasal and facial high-flow oxygen, as well as ensuring the availability of airway suctioning equipment and advanced airway equipment, including a videolaryngoscope and fibreoptic laryngoscope. Manual in-line stabilisation of the cervical spine is required if there is a history of trauma. A plan for rescue airway management and oxygenation in the event of a failed intubation should include availability of supraglottic airway devices, as well as surgical or percutaneous cricothyroidotomy techniques.(14-17) In our case series, all patients were intubated uneventfully using an RSI technique. Patients 2, 3 and 4 were deemed to require prophylactic intubation in the A&E in view of their altered mental status (Patients 2 and 4) or significant oedema on fibreoptic laryngoscopy (Patients 2 and 3). Patients 1 and 5 were considered stable for transfer to the EOT for endotracheal intubation, which is the case for the majority of our patients.
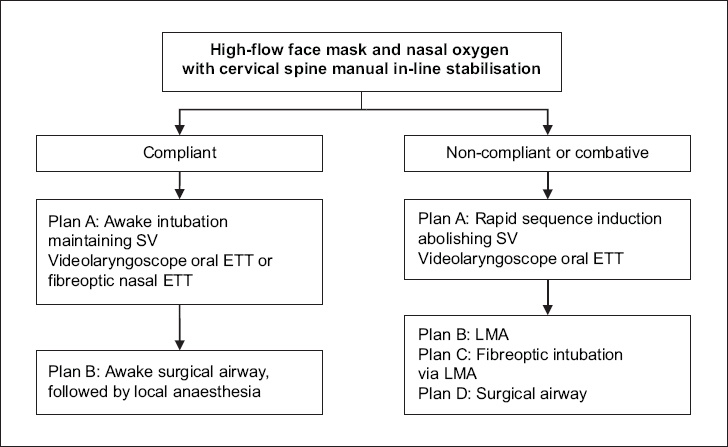
Patients with inhalation injury have a higher risk of failed intubation as well as a lower likelihood of successful rescue oxygenation and ventilation. In the event of failure or if there is any delay in securing the airway, we produced an aide-memoire (
Fig. 2
Flowchart shows the decision-making process for upper airway management in inhalation injury. ETT: endotracheal tube; LMA: laryngeal mask airway; SV: spontaneous ventilation
Fibreoptic bronchoscopy should only be performed after the airway is secured, ventilation is controlled and the patient’s condition is stabilised. Unless there is any refractory hypoxaemia or lobar collapse, urgent surgery for burns or trauma should be performed prior to diagnostic fibreoptic bronchoscopy. Bronchoalveolar lavage and suctioning should be performed to clear obstructed airways and to obtain samples for microbiology.
In Endorf and Gamelli’s(18) retrospective chart review over three years, 80 patients were identified with inhalation injury, which required intubation and mechanical ventilation as well as fibreoptic bronchoscopy in the first 24 hours. The bronchoscopic abbreviated injury score (AIS) of the patients was found to correlate with mortality. The AIS is a grading system for inhalation injury that is scored according to the presence of carbonaceous deposits, bronchorrhoea, erythema, oedema, mucosal friability, sloughing and necrosis, bronchial obstruction, and endoluminal obliteration. The overall AIS is graded according to the worst feature present in any category.(3) In our practice, however, we found that this may lead to differences in grading between different observers. Of particular note, there may be a difference between the severity and distribution of each component of the score, especially the degree of inflammation, degree of mucosal damage and carbonaceous deposits. This is illustrated in images from Patient 1 (
Fig. 3
Images of Patient 1 collected during his acute respiratory distress syndrome (ARDS) phase while in the BICU. Bronchoscopic images show (a) bronchorrhoea; and (b) bronchial mucosal erythema and bleeding. (c) Chest radiograph shows ARDS. (d) Photograph shows carbonaceous deposits extracted from bronchoalveolar lavage.
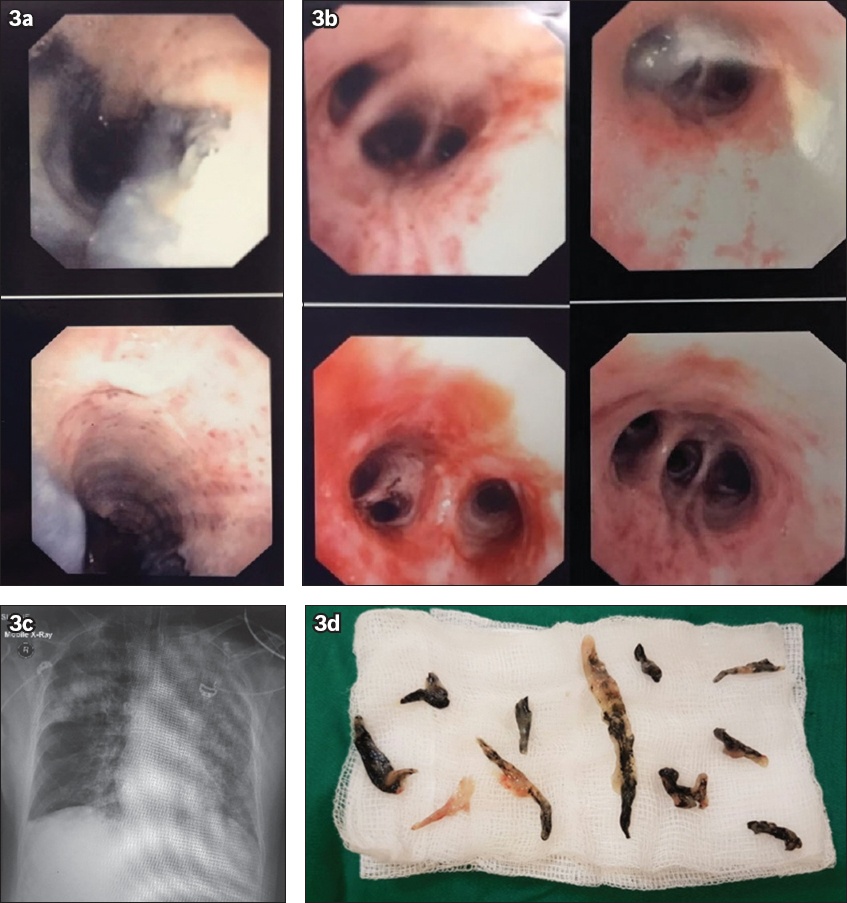
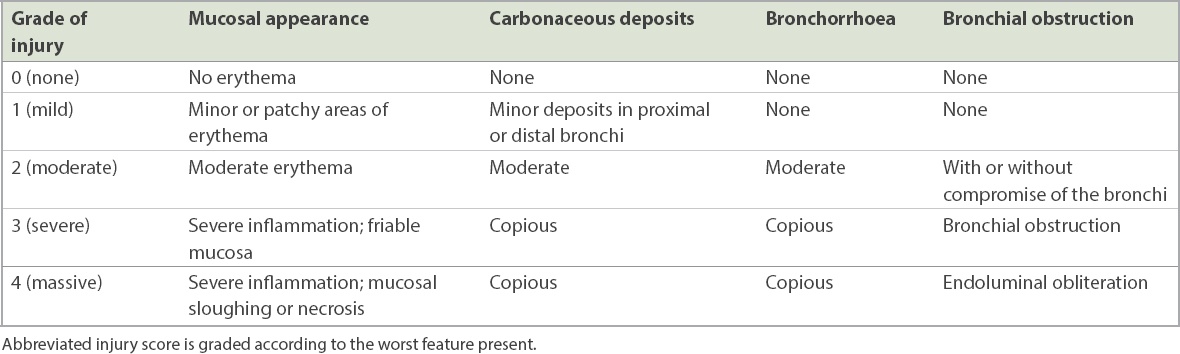
Table III
Modified Endorf and Gamelli classification separating components of the overall score for clarity.
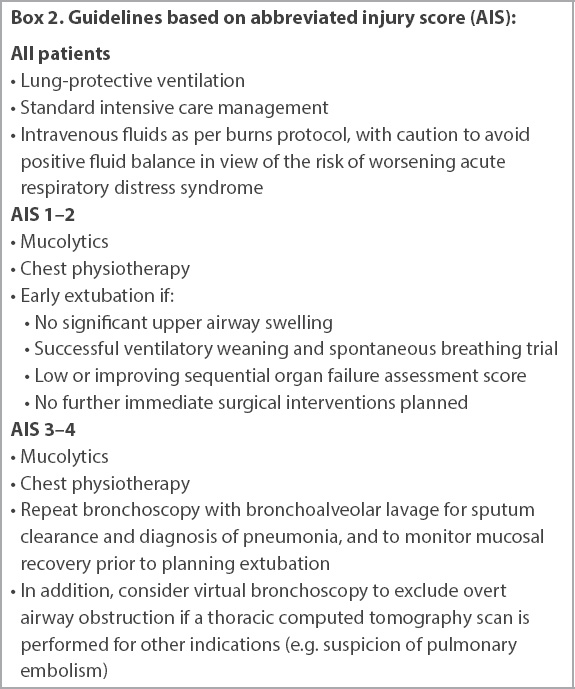
Lower airway fibreoptic bronchoscopic AIS is particularly useful in planning for early extubation following burns surgery in lower grades of injury (AIS 1–2) and predicting the need for more prolonged ventilation in higher grades of injury (AIS 3–4). AIS correlates with histologic findings of inhalation injury from bronchial biopsy, risk of ARDS, deteriorating oxygenation, higher COHb levels, prolonged ventilation, organ dysfunction and mortality.(19-23) In more severe cases, the need for repeat bronchoscopy for sputum clearance, bronchoalveolar lavage for the diagnosis of pneumonia, and monitoring mucosal recovery can be predicted.(24-26) Virtual bronchoscopy, from three-dimensional reconstructions of thoracic computerised tomography (CT) images, has a high negative predictive value for excluding airway narrowing and oedema in an animal model of inhalation injury.(27) In addition, virtual bronchoscopy was found to be reliable in confirming the diagnosis of inhalation injury in a small clinic study of ten patients.(28) It might be possible to apply this to the initial triage of patients in A&E, following upper airway fibreoptic laryngoscopy, to exclude overt airway obstruction with a high degree of reliability and minimise any delay in diagnosis. Virtual bronchoscopy may also play a role in patients in whom CT is being performed for other reasons, for example if there is coexisting trauma or suspicion of a pulmonary embolism. However, its limitations include the requirement for high-resolution CT image reconstruction and expertise in specialised image interpretation.
Hence, even though virtual bronchoscopy appears to be a promising diagnostic modality, further validation studies are required. In addition, it may not fully replace fibreoptic bronchoscopy, which has the advantage of allowing therapeutic suctioning of obstructing casts and the relief of life-threatening airway obstruction. Fibreoptic bronchoscopy has its own limitations, as it may prove challenging in hypoxic patients or if an endotracheal tube with a relatively narrow diameter is present. In our practice, we have introduced guidelines (
Box 2
Guidelines based on abbreviated injury score (AIS):
Another consideration is the use of nebulised heparin and acetylcysteine. Nebulised acetylcysteine has a potent mucolytic effect, but it is also a mild irritant, hence is traditionally administered together with bronchodilators to reduce the risk of bronchospasm. Bronchodilators may also be indicated in patients with severe inhalation injury or reactive airway disease (e.g. asthma or chronic obstructive pulmonary disease). Nebulised heparin is thought to be beneficial in inhalation injury by reducing fibrin cast formation and bronchial obstruction. Studies have demonstrated a reduction in ventilator days with no adverse bleeding events in inhalation injury patients treated with nebulised heparin in combination with acetylcysteine and bronchodilators. The optimal dose of nebulised heparin has been identified as 10,000 U every four hours.(29-31)
In making a decision regarding extubation, an airway plan must be formulated to decide whether to keep the patient intubated or consider early extubation according to conventional clinical criteria, including upper airway patency, neurological status, muscular weakness, respiratory secretions and chest compliance. In cases of resolving upper airway swelling, it may be helpful to plan extubation according to the presence of a positive endotracheal tube cuff leak test. A short course of dexamethasone may help to reduce swelling and extubation, while leaving an airway exchange catheter in situ may confer an additional degree of safety.(32) Application of facial continuous positive airway pressure or non-invasive ventilation via a tight-fitting face mask may not be possible in patients with facial burns; however, high-flow humidified oxygen therapy via nasal cannulae following extubation is emerging as a suitable alternative in other areas of critical care.(33,34) Specific factors to consider prior to extubation include the presence of: (a) upper airway thermal injury or swelling; (b) lower airway thermal injury or ARDS and whether further bronchoscopy is required to clear carbonaceous plugs; (c) bronchospasm; (d) pneumonia; (e) further surgery required; (f) ICU severity of illness and trends; (g) coexisting traumatic injuries or surgical/medical conditions; and (h) comorbidity, frailty and functional capacity.
Smailes et al(35) retrospectively reviewed the incidence of extubation failure in a cohort of patients managed in a tertiary BICU and requiring mechanical ventilation for longer than 24 hours. Of 60 patients planned to be extubated, 20 (33.3%) failed this and required reintubation within 48 hours. There was no significant difference in severity of inhalation injury and burn size in patients who were successfully or unsuccessfully extubated. Patients who failed extubation had a longer overall duration of mechanical ventilation as well as longer intensive care and hospital lengths of stay. In 15 (75.0%) out of 20 patients, impaired clearance of secretions was found to be a major risk factor for extubation failure.
In a separate study, Smailes et al(36) determined that a weak cough as well as copious respiratory secretions were major aetiological factors in burns patients requiring reintubation following a successful spontaneous breathing trial. While tracheostomy may be beneficial in facilitating ventilatory weaning and pulmonary toilet, it is associated with a high incidence of complications including a high incidence of subglottic stenosis in patients with moderate to severe inhalation injury.(37) At present, there is no consensus on the indications and timing for tracheostomy in this group of patients, and decisions must be made after considering the balance of risks and benefits in the individual patient.
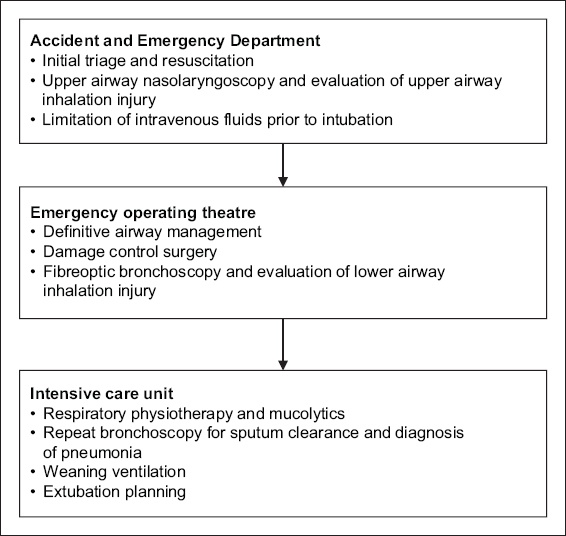
In conclusion, inhalation injury results in specific complications related to airway management. Based on our current case series and literature reviews, we propose the use of a standardised approach to management for this group of patients (
Fig. 4
Flowchart shows our recommended standardised workflow for patients with inhalation injury.