Singapore Med J 2022; 63(3): 118-124 doi: 10.11622/smedj.2022044
Artificial intelligence-assisted colonoscopy: a narrative review of current data and clinical applications
James Weiquan Li1,2,3, FRCPEdin, FAMS, Lai Mun Wang4,5, FRCPath, FRCPEdin, Tiing Leong Ang1,2,3, FRCPEdin, FAMS
Author Information >Copyright and License information >
1Department of Gastroenterology and Hepatology, Changi General Hospital, Singapore 2Yong Loo Lin School of Medicine, National University of Singapore, Singapore 3SingHealth Duke-NUS Medicine Academic Clinical Programme, Singapore 4Pathology Section, Department of Laboratory Medicine, Changi General Hospital, Singapore 5SingHealth Duke-NUS Pathology Academic Clinical Programme, Singapore Correspondence: Clinical Asst Prof James Weiquan Li, Department of Gastroenterology and Hepatology, Changi General Hospital, 2 Simei Street 3, Singapore 529889. james.li.w.q@singhealth.com.sg
Colonoscopy is the reference standard procedure for the prevention and diagnosis of colorectal cancer, which is a leading cause of cancer-related deaths in Singapore. Artificial intelligence systems are automated, objective and reproducible. Artificial intelligence-assisted colonoscopy has recently been introduced into clinical practice as a clinical decision support tool. This review article provides a summary of the current published data and discusses ongoing research and current clinical applications of artificial intelligence-assisted colonoscopy.
Colorectal cancer (CRC) is the most frequently occurring cancer and a leading cause of cancer-related mortality in Singapore.(1) Colonoscopy is the reference standard procedure for the prevention and diagnosis of CRC and has been shown to reduce CRC-related mortality.(2,3) The role of colonoscopy in the prevention of CRC lies in the accurate detection and adequate resection of colorectal adenomas that are considered premalignant and may progress to CRC. A 1% increase in adenoma detection rate (ADR) has been shown to reduce interval CRC by 3%.(4) The adequacy of resection largely depends on the appropriate choice of technique and endoscopic accessories, which, in turn, is dependent on the size, morphology, predicted histology and, in cases of early cancer, the predicted depth of invasion.(5,6) The same factors and adequacy of resection determine the risk of recurrence of colorectal adenomas and influence the timing of surveillance colonoscopy.(7,8)
Artificial intelligence (AI) comprises several different fields. Machine learning and, more specifically, deep learning, in which hierarchical representation learning is performed across multiple layers of artificial neural networks,(9) is the most extensively studied application of AI in medicine.(10) Most research on AI in gastroenterology has centred on addressing the unmet needs in colonoscopy, with the goal of reducing CRC-related morbidity and mortality.(11,12) Position statements and recommendations regarding AI in endoscopy have been published, and they serve to facilitate and regulate the proliferation of research on the use of AI in endoscopy practice.(13-15)
The use of AI in colonoscopy in now a clinical reality, as AI systems have received regulatory approval and are now commercially available. Robust data in the context of polyp and adenoma detection has been published, but research on its utility in disease differentiation and quality assurance is ongoing. This narrative review article aims to provide a summary of current published data and clinical applications of AI-assisted colonoscopy. It focuses on areas of unmet needs that are of clinical significance and highlights the potential role of AI in filling the current gaps in colonoscopy.
LITERATURE SEARCH
A comprehensive literature search was performed in the PubMed, Web of Science, MEDLINE and EMBASE electronic databases from the inception of the databases up to and including 5 December 2021. The key search terms used were ‘artificial intelligence’ OR ‘deep learning’ OR ‘computer aided detection’ OR ‘computer aided diagnosis’ AND ‘colonoscopy’. Electronic searches were supplemented with manual searches of references of all retrieved studies to identify other relevant publications, and only studies published in English were considered for this narrative review article.
COMPUTER-AIDED DETECTION FOR POLYP DETECTION IN COLONOSCOPY
CRCs detected after a prior colonoscopy and in the interval between scheduled surveillance colonoscopies are known as interval cancers or post-colonoscopy CRCs (PCCRCs). PCCRCs may be due to the biological behaviour of the CRC, or missed or incompletely resected adenomas. It is estimated that the incidence of interval CRC is as high as 3.5 per 1,000 screened persons.(16) An earlier study found that 52% of PCCRCs were attributable to probable missed lesions, while 19% of PCCRCs in the study may possibly be related to incompletely resected lesions.(17) In a more recent study conducted in a national colonoscopy training centre, where World Endoscopy Organization (WEO) methodology was used to determine and categorise PCCRCs, it was deemed that 85% of CRC cases after a negative colonoscopy were due to possible missed lesions according to the WEO criteria.(18) Zhao et al conducted a meta-analysis of more than 15,000 tandem colonoscopies and found that the adenoma miss rate (AMR) was 26% (95% confidence interval [CI] 23%–30%).(19)
Although AMR may be influenced by several factors, an important determinant of AMR is the endoscopist,(20,21) as an inability to maintain a sustained level of alertness during colonoscopy owing to distraction and fatigue may result in a polyp being missed despite it being visible on the monitor. The inclusion of nurses and endoscopy trainees during colonoscopy has been shown to increase ADR, as they act as an independent ‘second reader’ to the endoscopist.(22,23) Computer-aided detection (CADe) functions as an automated second reader, but without the inherent problems of distraction and fatigue that may affect the performance of the endoscopist and the human second reader.
In a meta-analysis(24) consisting of five randomised controlled trials (RCTs)(25-29) with 4,354 patients, the pooled ADR was significantly higher in the CADe group than in the control group (36.6% vs 25.2%, relative risk [RR] 1.44, 95% CI 1.27–1.62; p < 0.01), with both groups using high-definition white light endoscopes. There was no significant difference in the withdrawal times between the groups in the individual trials, which eliminated the possibility of withdrawal time acting as a confounder for the efficacy of the CADe systems in increasing ADR. However, it must be noted that the increase in ADR with CADe was almost entirely due to the increased detection of diminutive (< 5 mm) adenomas, with only one study(27) showing an improvement in detection of small (6–9 mm) adenomas (17.2% vs. 12.7%; p < 0.05) and none of the studies showing a difference in the detection of advanced adenomas > 10 mm. Up to 90% of polyps detected during colonoscopy are diminutive and small in size, and the rates of progression of these lesions to CRC are thought to be low.(30) A recently conducted large-scale, propensity score-matched, single-centre prospective study on 1,836 patients in Japan(31) similarly showed an increase in ADR with CADe compared to controls (26.4% vs. 19.9%). However, most of this increase in ADR was for diminutive polyps, with no significant increase observed in detection of advanced neoplasia (3.7% vs. 2.9%, respectively). This data is consistent with prior publications related to polyp size and miss rate. A systematic review by van Rijn et al examined miss rates based on the size of the polyp.(32) The AMR for adenomas > 10 mm, 5–10 mm and 1–5 mm was 2.1% (95% CI 0.3%–7.3%), 13% (95% CI 8.0%–18%) and 26% (95% CI 27%–35%), respectively. Although small polyps are usually benign and do not progress, about 6% of such polyps have been shown to progress to advanced adenomas over time.(30) Small adenomas have also been shown to harbour foci of high-grade dysplasia or intramucosal cancer.(33) The recommended surveillance interval following colonoscopy and endoscopic resection of colonic adenomas is 1–10 years, based on the numbers of adenomas, as well as the histology.(7) Hence, small adenomas cannot be simply dismissed and are of potential clinical relevance. Apart from size, a flat or mildly elevated polyp morphology, such as in the context of serrated polyps, has also been implicated as a factor for missed lesions.(19) CADe has been demonstrated to increase the detection of adenomas of both flat (RR 1.78, 95% CI 1.47–2.15) and polypoid morphology (RR 1.54, 95% CI 1.40–1.68).(24)
Livovsky et al(34) studied the Detection of Elusive Polyps (DEEP2) polyp detection system, specifically looking at the performance of CADe in detecting elusive polyps, which were divided into fleeting and subtle polyps in the study. Fleeting polyps were defined as polyps appearing in the field of view (FOV) for ≤ 5 seconds, while subtle polyps were those missed initially by the endoscopist and offline independent gastroenterologists who were reviewing recorded videos of the colonoscopy for annotation purposes. The study found that when polyps appeared in the FOV for < 5 seconds, the sensitivity of DEEP2 for detection was 88.5% (95% CI 84.6%–92.4%), compared to 31.7% (95% CI 26.0%–37.5%) for the endoscopist (p < 0.01). The difference in sensitivity was 84.9% (95% CI 79.3%–90.5%) versus 18.9% (95% CI 12.8%–24.9%), respectively, when the FOV was adjusted to < 2 seconds. The study also showed that DEEP2 was able to detect an average of 0.22 subtle polyps per sequence.
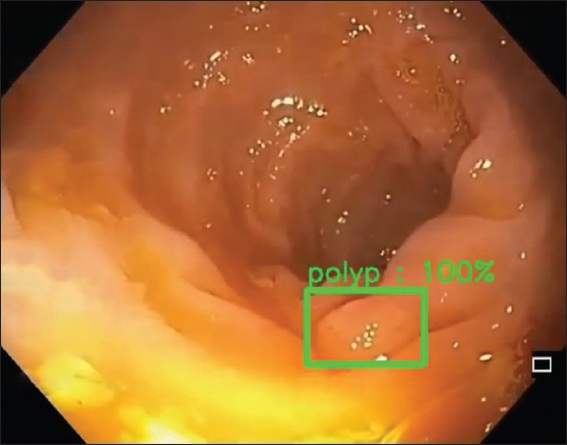
Tandem colonoscopy studies on CADe shed some light into its impact on AMR. In a prospective tandem colonoscopy study conducted by Wang et al,(35) patients were randomly assigned to colonoscopy with or without CADe, which was immediately followed by the other procedure. The AMR was significantly lower in the group that underwent colonoscopy with CADe compared with routine colonoscopy as the first procedure (13.9% vs. 40.0%; p < 0.0001). This result was consistent regardless of the segment of the colon examined. The CADeT-CS Trial(36) was a prospective, multicentre, single-blind, randomised tandem colonoscopy study conducted in a United States population, which also showed a decrease in AMR in the CADe-first group compared to the high-definition white light group (20.12% vs. 31.25%; odds ratio [OR] 1.8048, 95% CI 1.0780–3.0217; p = 0.0247). In another study by Lui et al,(37) the colon was divided into different segments for withdrawal and the endoscopist was blinded to the CADe output, which was displayed on a separate monitor. Unblinding of AI results for the endoscopist was provided by an independent viewer after each colonic segment was examined. Using this method, the total number of polyps and adenomas detected increased by 32.1% and 23.6%, respectively. An example of CADe in real-time colonoscopy is shown in Fig. 1.
Fig. 1
Colonoscopy image shows the use of computer-aided detection, in which the polyp is highlighted in a bounding box displayed in real time on the endoscopy monitor.
Despite the apparent advantages of CADe in increasing polyp detection and reducing AMR, AI systems also suffer from the same limitations as expert endoscopists. Polyps that are not visible on the endoscopy monitor will be ‘invisible’ to polyp detection systems. This could be due to being hidden behind mucosal folds or concealed by poor bowel preparation. In a study that evaluated false detections with CADe in colonoscopy,(38) blurry images were found to result in distorted polyp texture and were one of the reasons for false negative detections. These false negative detections also occurred when polyps approached the corner of a frame just before appearing or disappearing from the FOV. In addition, false positive detections increase the amount of visual distraction experienced by the endoscopist. The impact of this is not fully known, as the majority of early studies on CADe do not explicitly report or analyse false positive detections. There has been an effort to define the false positive duration of a frame before it should be considered a false positive detection,(39) but this has not been adequately studied and no consensus has been reached on an acceptable definition.
COMPUTER-AIDED DIAGNOSIS FOR POLYP CHARACTERISATION DURING COLONOSCOPY
Various polyp classification systems have been developed for in vivo prediction of polyp histology before resection and formal histological analysis. Also known as an optical biopsy, these systems exploit the different appearances of polyp surfaces and vessels under narrow-band wavelengths of light(40) or when stained with dyes(41) to determine their neoplastic potential and estimated depth of invasion, and are collectively known as image-enhanced endoscopy (IEE). Narrow-band imaging (NBI) and blue laser imaging (BLI) are the most extensively studied examples of IEE utilising narrowed wavelengths of white light. As discussed in the introduction, the predicted histology of colorectal polyps aids the endoscopist in selecting the optimal method of resection. The optical prediction of polyp histology is also a crucial element of the ‘resect and discard’(42,43) and ‘detect and leave’(44) strategies, which can make endoscopic examinations and treatment of diminutive colorectal polyps more cost-effective, provided these satisfy the criteria of the American Society for Gastrointestinal Endoscopy (ASGE) Preservation and Incorporation of Valuable endoscopic Innovations (PIVI) recommendations. This requires that in the context of suspected rectosigmoid hyperplastic polyps that are 5 mm or smaller, the technology should provide a negative predictive value (NPV) greater than 90%, when used with high confidence, for adenomatous histology.(45) Examples of IEE classification include the Kudo pit pattern,(41) Sano,(46) NBI International Colorectal Endoscopic,(47) Japan NBI Expert Team(48) and BLI Adenoma Serrated International Classification(49) systems.
The use of IEE in clinical practice is dependent on the availability of equipment, the experience of the endoscopist and access to structured training. While the latter has been shown to improve the accuracy of optical biopsy with IEE,(50) there is still a wide gap in accessibility to proper equipment and training depending on the resources available. This has resulted in moderate interobserver variability(51,52) and modest results(53) where accuracy of IEE for prediction of polyp histology has been studied in clinical practice.
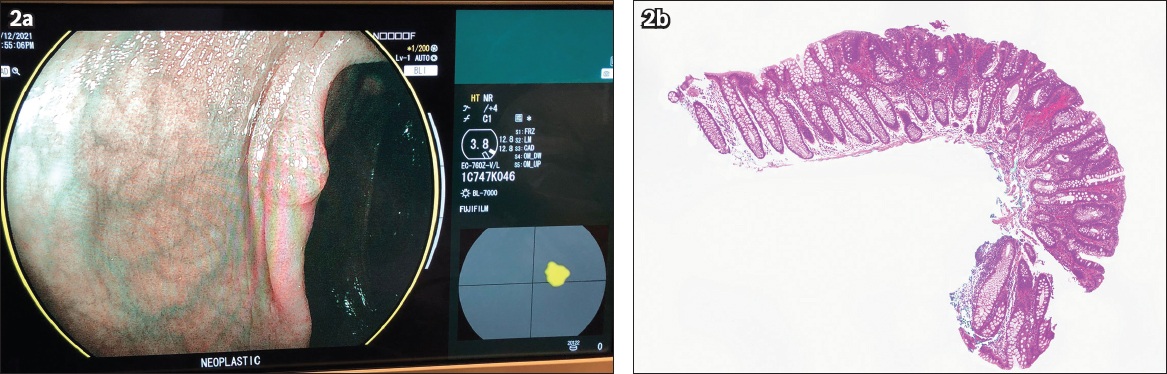
Most of the early studies evaluating computed-aided diagnosis (CADx) were retrospective in nature and tested deep learning models on still images or video recordings of polyps.(54-58) In contrast, few prospective studies on CADx in real-time colonoscopy are currently available. In a study comparing magnifying NBI and a CADx support vector machine in 118 colorectal lesions, Kominami et al(59) were able to demonstrate a concordance between the endoscopic diagnosis and CADx output of 97.5%. The accuracy, sensitivity, specificity, positive predictive value (PPV) and NPV of the CADx system’s output were 94.9%, 95.9%, 93.3%, 95.9% and 93.3%, respectively. Song et al(60) used a deep learning model to classify near-focus NBI images of polyps in real-time. The study showed that the CADx system was able to classify polyps as serrated polyps, benign adenomas/mucosal/superficial submucosal cancer and deep submucosal cancer, with areas under the receiver operating characteristic curve (AUROC) of 0.93–0.95, 0.86–0.89 and 0.89–0.91, respectively. CADx had an overall diagnostic accuracy of 81.3%–82.4%, which outperformed trainee endoscopists and was comparable with that of expert endoscopists. When CADx was used to assist trainee endoscopists, an increase in agreement was observed between true and predicted polyp histology (kappa improved from 0.368 to 0.655), while the diagnostic accuracy increased from 63.8%–71.8% to 82.7%–84.2%. A meta-analysis(61) of 18 studies (three prospective, 15 retrospective, total of 7,680 polyp images) on prediction of polyp histology using CADx models showed a pooled sensitivity, specificity and AUROC of 92.3% (95% CI 88.8%–94.9%), 89.8% (95% CI 85.3%–93.0%) and 0.96 (95% CI 0.95–0.98), respectively. Six of the included studies compared the performance of CADx with non-expert endoscopists and showed that CADx was significantly better than non-expert endoscopists in the accurate prediction of polyp histology (AUC 0.97 vs 0.90, respectively; p < 0.01). Fig. 2 is an example of CADx with corresponding endoscopic and histology images.
Fig. 2
(a) Colonoscopy image shows the use computer-aided diagnosis to predict a neoplastic polyp. (b) Photomicrograph shows a tubular adenoma with low-grade dysplasia (Haematoxylin & eosin, original magnification × 40).
CADx has also been studied with endocytoscopy, which utilises specialised contact light microscopy colonoscopes with 520× optical zoom capability and mucosal staining techniques to visualise cellular structures. A single-centre, open-label, prospective study(62) showed that endocytoscopy with CADx had an NPV for diminutive rectosigmoid adenomas of 93.7%–96.4% with methylene blue staining and 95.2%–96.5% with NBI, which satisfied the ‘detect and leave’ threshold of 90% recommended by the ASGE PIVI.(45) Rodriguez-Diaz et al(63) used a CADx model that simultaneously displayed elements informing polyp histology assessment in each frame on the endoscopy monitor. The model output was a detailed spatial histology heat map using varying shades of red, green and yellow to represent high-confidence neoplastic, high-confidence non-neoplastic and low-confidence assessments, respectively. This augmented visualisation of the polyp in real-time enabled the endoscopist to assess the prediction made and use the spatial information to guide decisions on management of the polyp in question. The CADx model was tested on 254 polyps, with a sensitivity, specificity and NPV of 96%, 84% and 91%, respectively, in distinguishing neoplastic from non-neoplastic polyps of all sizes.
AI-ASSISTED QUALITY ASSURANCE IN COLONOSCOPY
Owing to its unique role in the prevention of CRC, strict quality indices have been recommended to ensure that all screening colonoscopies are of high quality.(2,3) These quality indices include not only the ADR of the endoscopist but also the withdrawal time,(64) caecal intubation rate and adequacy of bowel preparation.(65,66) Despite being extensively studied, quality indices in performance and reporting of colonoscopy may not be adhered to because of lack of real-time feedback, training and enforcement.(67,68) For example, most endoscopists are unaware of their individual ADR. This could be due to a variety of factors including the manual nature of collecting and combining information from colonoscopy and histology reports, which are recorded on separate electronic systems or in hard copy in virtually all centres, as well as lack of regular and structured feedback on the individual endoscopist’s ADR. A recent study conducted in Japan(69) showed that a group meeting and individual interview with the director to communicate endoscopist performance in ADR could increase the mean ADR significantly from 40.8% to 50.8%. This example highlights how feedback on the individual quality indices in colonoscopy could improve the endoscopist’s performance in colonoscopy.
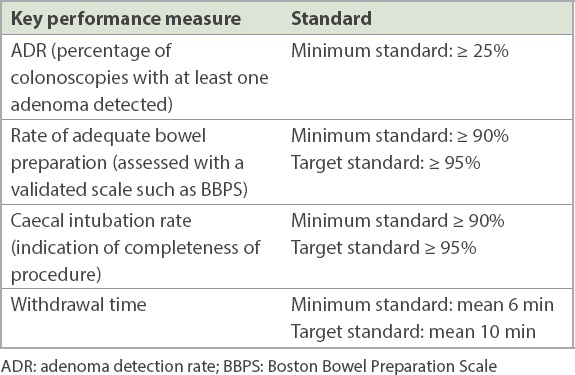
Gong et al(70) conducted an RCT of 704 patients using the ENDOANGEL system, which provided automated monitoring of withdrawal time and speed, and adequacy of mucosal exposure. The information was relayed to the endoscopist in real time and resulted in a significantly longer mean withdrawal time in the ENDOANGEL group compared to the control group (6.38 minutes vs. 4.76 minutes, respectively; p < 0.001). The ADR in the ENDOANGEL group was significantly higher (16% vs. 8%), and this is currently the only RCT to show an increased detection rate in adenomas > 10 mm in size (10/355 vs. 1/349, respectively; OR 9.50, 95% CI 1.19–75.75; p = 0.034). The use of an automatic quality control system (AQCS) was also shown to improve mean withdrawal times from 5.68 minutes to 7.03 minutes (p < 0.001) in a study by Su et al.(28) The AQCS generated audio prompts for the endoscopist to slow down the speed of withdrawal when unstable or blurry frames were displayed, or when a colonic segment had a suboptimal bowel preparation with Boston Bowel Preparation Scale (BBPS) < 2. Using this automated system, the rate of bowel preparation was also increased (87.3% vs. 80.6%, p = 0.023). The AQCS was combined with CADe in the study and showed an increase in ADR (28.9% vs. 16.5%, p < 0.001). However, it should be noted that in both these studies, the control groups did not meet the minimum standard for withdrawal time and ADR (Table I). The ADR in the ENDOANGEL group in the former study was also far below what is expected.(2,3) Hence, the role of these systems in centres and among experienced endoscopists where such quality indices are already adhered to is unclear.
Table I
Examples of quality indicators in colonoscopy.
The use of deep learning for automatic calculation of the BBPS in colonoscopy was also examined in a prospective observational study.(71,72) The automatic BBPS (e-BBPS) system was based on existing definitions of adequacy of bowel preparation spelled out in the BBPS. It was prospectively validated in 616 patients undergoing screening colonoscopy and showed a significant inverse correlation between the e-BBBPS score and ADR (Spearman’s rank correlation −0.976; p < 0.01). Based on the results of the study, a threshold e-BBPS score of 3 was calculated to guarantee an ADR of more than 25%. Using this threshold, patients with an e-BBPS score of ≤ 3 had a significantly higher ADR than patients with e-BBPS > 3 (28.03% vs. 15.93%; p < 0.001). The study showed that a validated AI system based on deep learning can supplement the endoscopist with objective and precise information about bowel preparation that is reproducible and more refined than current visual estimations of bowel preparation by the endoscopist.
Yao et al examined the role of combined CADe and computer-aided quality improvement system (CAQ) during colonoscopy in improving ADR.(73) Patients undergoing colonoscopy were randomised to four groups: (control: 271, CADe: 268, CAQ: 269 and CADe plus CAQ [COMBO]: 268). The primary outcome was ADR. The average ADR in the control, CADe, CAQ and COMBO groups was 14.76% (95% CI 10.54%–18.98%), 21.27% (95% CI 16.37%–26.17%), 24.54% (95% CI 19.39%–29.68%) and 30.6% (95% CI 25.08%–36.11%), respectively. The ADR was significantly higher in the COMBO group than in the CADe group (30.60% vs. 21.27%; p = 0.024), but the difference was not significantly different when compared to the CAQ group (30.60% vs. 24.54%; p = 0.213).
To overcome the inefficient and time-consuming nature of manual data retrieval and tracking of patients for post-polypectomy colonoscopy surveillance, a pipeline utilising natural language processing (NLP) techniques was developed to automatically extract and analyse information from free-text colonoscopy and pathology reports.(74) The pipeline consisted of three modules. The first module was for polyp property extraction, where rule-based methods and statistical classifiers were used to extract relevant information about polyps from colonoscopy and histology reports. In the polyp grouping module, extracted polyp properties such as morphology, location and size were associated with their unique polyp mentions. Lastly, the surveillance interval classification module integrated the information to classify patients into one of six risk categories based on the recommended post-colonoscopy surveillance intervals by the United States Multi-Society Task Force on CRC.(7) The pipeline was evaluated on an independent test set of 200 reports (100 each from colonoscopy and histology) and achieved an overall accuracy of 92% in assigning the recommended interval for surveillance colonoscopy. The study showed that NLP techniques can be used in colonoscopy to develop a pipeline for automated assignment of surveillance intervals, which has traditionally been a very tedious and inefficient process.
OTHER EXAMPLES OF RESEARCH IN THE USE OF AI IN COLONOSCOPY
The same principles of objectivity and reproducibility with automated systems discussed in this review article can also be applied to other areas of colonoscopy. For example, colonoscopy is an essential tool in the diagnosis and assessment of severity of inflammatory bowel disease (IBD). However, endoscopic assessment has inherent subjectivity, which is further compounded by differences in training, volume of cases seen and the level of expertise of the individual endoscopist. In this setting, AI systems have been studied to more reliably diagnose and assess disease severity in IBD.(75-77)
Similarly, the estimation of CRC depth and risk of lymph node metastasis is crucial in determining whether endoscopic resection techniques such as endoscopic submucosal dissection and endoscopic mucosal resection are appropriate to achieve curative resection, which has lower associated morbidity and mortality compared to surgical resection.(78-81) Accurate prediction of depth of CRC invasion in real time, as well as determination of risk of lymph node metastasis in T1 CRC, can be very challenging for clinicians.(82-84) It is, therefore, unsurprising that AI is also being studied in these areas.(85-87)
INTEGRATING AI-ASSISTED COLONOSCOPY INTO CURRENT CLINICAL PRACTICE
Current commercially available AI systems in Singapore either have the CADe function alone or CADe combined with CADx functions. The current CADx function differentiates between hyperplastic and neoplastic polyps. There is no further stratification in terms of severity of dysplasia or depth of invasion in the context of cancer. Therefore, it would appear that the current key utility of AI-assisted colonoscopy is its role in increasing ADR, thereby facilitating diagnosis and endoscopic resection of adenomas that may otherwise be missed. This is especially useful for less experienced endoscopists performing screening colonoscopy. Admittedly, there is no direct data on the longer-term impact of CADe in terms of reduction in CRC incidence and CRC-related mortality, but these are reasonable assumptions to extrapolate from past data related to screening colonoscopy.(4) ADR is a function of different components during the process of colonoscopy, and it is important and illustrative to dissect these individual components in order to better appreciate how to improve ADR using different approaches. Excellent mucosa surface visibility is extremely important for adenoma detection, and it depends on the adequacy of bowel preparation, and irrigation and suctioning during the process of colonoscopy. Another crucial aspect is meticulous examination of the entire visible colonic mucosa (careful slow withdrawal of the endoscope, adequate air insufflation, pressing down and looking behind folds, and re-examination of flexures). The third vital element is being aware that premalignant lesions such as sessile serrated adenomas may be easily missed owing to their subtle endoscopic features, and being trained to recognise such subtle features and detect these flat subtle lesions on the exposed mucosa surface. Different endoscopic tools are available to improve adenoma detection, focusing on different aspects of the examination process during colonoscopy. These include devices attached to the colonoscopy tip to flatten mucosal folds in order to expose adenomas hidden by folds; contrast dye-based IEE techniques such as indigo carmine chromoendoscopy, which accentuates mucosal surface contours to highlight flat lesions; electronic IEE techniques such as NBI and BLI that accentuate mucosal surface details to facilitate recognition of subtle mucosal surface abnormalities to improve detection, and with additional magnification, also allow characterisation and diagnosis; and endoscopy systems such as full-spectrum endoscopy (FUSE) that increase the extent of the endoscopic view.(88) CADe draws the endoscopist’s attention to the presence of a polyp when it appears in the endoscopic view. However, it will not be able to detect polyps in unexposed areas, such as when they are hidden behind mucosal folds or obscured owing to suboptimal bowel preparation, and when the colonoscope withdrawal speed is too fast.
A recent network meta-analysis of 50 RCTs comprising 34,445 participants compared CADe with high-definition white light endoscopy, IEE techniques, and techniques that increased mucosal visualisation such as distal attachments and FUSE.(89) CADe was ranked as the superior technique for adenoma detection. Cross-comparisons of CADe with other imaging techniques showed a significant increase in the ADR with CADe versus increased mucosal visualisation systems (OR 1.54 [95% CI 1.22–1.94]; low certainty of evidence) and with CADe versus chromoendoscopy (OR 1.45 [95% CI 1.14–1.85]; moderate certainty of evidence). CADe also seemed to be the superior strategy for detection of sessile serrated lesions (with moderate confidence in hierarchical ranking), although no significant increase in the sessile serrated lesion detection rate was observed (OR 1.37 [95% CI 0.65–2.88]).
CONCLUSION
The role of AI-assisted colonoscopy is expanding, with data and clinical applications emerging most rapidly in the fields of polyp detection, prediction of polyp histology and automated quality assurance. The objectivity and reproducibility afforded by these automated systems will see a further expansion of data from AI-assisted colonoscopy in other areas of colonoscopy and newer clinical applications. We should harness advances in technology to improve our practice. However, we should also keep in mind that technology complements but does not replace the fundamentals of quality colonoscopy.
References National Registry of Diseases OfficeSingapore Cancer Registry Annual Report 2018. Available at: https://www.nrdo.gov.sg/docs/librariesprovider3/default-document-library/scr-annual-report-2018.pdf. Accessed March 31, 2021. Kaminski MF, Thomas-Gibson S, Bugajski M, et al. Performance measures for lower gastrointestinal endoscopy:a European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative.Endoscopy. 2017;49:378-97. Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy.Gastrointest Endosc. 2015;81:31-53. Corley DA, Levin TR, Doubeni CA.Adenoma detection rate and risk of colorectal cancer and death.N Engl J Med. 2014;370:2541. Kaltenbach T, Anderson JC, Burke CA, et al. Endoscopic removal of colorectal lesions-recommendations by the US Multi-Society Task Force on Colorectal Cancer.Gastroenterology. 2020;158:1095-1129. Ang TL, Lim JF, Chua TS, et al. Clinical guidance on endoscopic management of colonic polyps in Singapore.Singapore Med J. 2020;https://doi.org/10.11622/smedj.2020108[Epub ahead of print]. Gupta S, Lieberman D, Anderson JC, et al. Recommendations for follow-up after colonoscopy and polypectomy:a consensus update by the US Multi-Society Task Force on Colorectal Cancer.Gastrointest Endosc. 2020;91:463-85.e5. Hassan C, Antonelli G, Dumonceau JM, et al. Post-polypectomy colonoscopy surveillance:European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Update 2020.Endoscopy. 2020;52:687-700. Shalev-Shwartz S. Understanding Machine Learning:from Theory to Algorithms. 2014;New York Cambridge University Press. Kaul V, Enslin S, Gross SA.History of artificial intelligence in medicine.Gastrointest Endosc. 2020;92:807-12. Li JW, Ang TL.Colonoscopy and artificial intelligence:Bridging the gap or a gap needing to be bridged?.Artif Intell Gastrointest Endosc. 2021;2:36-49. Chen H, Sung JJY.Potentials of AI in medical image analysis in Gastroenterology and Hepatology.J Gastroenterol Hepatol. 2021;36:31-8. Ahmad OF, Mori Y, Misawa M, et al. Establishing key research questions for the implementation of artificial intelligence in colonoscopy:a modified Delphi method.Endoscopy. 2021;53:893-901. Berzin TM, Parasa S, Wallace MB, et al. Position statement on priorities for artificial intelligence in GI endoscopy:a report by the ASGE Task Force.Gastrointest Endosc. 2020;92:951-9. Bisschops R, East JE, Hassan C, et al. Advanced imaging for detection and differentiation of colorectal neoplasia:European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Update 2019.Endoscopy. 2019;51:1155-79. Pohl H, Robertson DJ.Colorectal cancers detected after colonoscopy frequently result from missed lesions.Clin Gastroenterol Hepatol. 2010;8:858-64. Robertson DJ, Lieberman DA, Winawer SJ, et al. Colorectal cancers soon after colonoscopy:a pooled multicohort analysis.Gut. 2014;63:949-56. Anderson R, Burr NE, Valori R.Causes of post-colonoscopy colorectal cancers based on World Endoscopy Organization System of Analysis.Gastroenterology. 2020;158:1287-99.e2. Zhao S, Wang S, Pan P, et al. Magnitude, risk factors, and factors associated with adenoma miss rate of tandem colonoscopy:a systematic review and meta-analysis.Gastroenterology. 2019;156:1661-74.e11. Rex DK, Cutler CS, Lemmel GT, et al. Colonoscopic miss rates of adenomas determined by back-to-back colonoscopies.Gastroenterology. 1997;112:24-8. Leufkens AM, van Oijen MGH, Vleggaar FP, Siersema PD.Factors influencing the miss rate of polyps in a back-to-back colonoscopy study.Endoscopy. 2012;44:470-5. Lee CK, Park DI, Lee SH, et al. Participation by experienced endoscopy nurses increases the detection rate of colon polyps dang a screening colonoscopy:a multicenter, prospective, randomized study.Gastrointest Endosc. 2011;74:1094-102. Buchner AM, Shahid MW, Heckman MG, et al. Trainee participation is associated with increased small adenoma detection.Gastrointest Endosc. 2011;73:1223-31. Hassan C, Spadaccini M, Iannone A, et al. Performance of artificial intelligence in colonoscopy for adenoma and polyp detection:a systematic review and meta-analysis.Gastrointest Endosc. 2021;93:77-85.e6. Wang P, Berzin TM, Glissen Brown JR, et al. Real-time automatic detection system increases colonoscopic polyp and adenoma detection rates:a prospective randomised controlled study.Gut. 2019;68:1813-9. Wang P, Liu X, Berzin TM, et al. Effect of a deep-learning computer-aided detection system on adenoma detection dang colonoscopy (CADe-DB trial):a double-blind randomised study.Lancet Gastroenterol Hepatol. 2020;5:343-51. Repici A, Badalamenti M, Maselli R, et al. Efficacy of real-time computer-aided detection of colorectal neoplasia in a randomized trial.Gastroenterology. 2020;159:512-20.e7. Su JR, Li Z, Shao XJ, et al. Impact of a real-time automatic quality control system on colorectal polyp and adenoma detection:a prospective randomized controlled study (with videos).Gastrointest Endosc. 2020;91:415-24.e4. Liu WN, Zhang YY, Bian XQ, et al. Study on detection rate of polyps and adenomas in artificial-intelligence-aided colonoscopy.Saudi J Gastroenterol. 2020;26:13-9. Vleugels JLA, Hazewinkel Y, Fockens P, Dekker E.Natural history of diminutive and small colorectal polyps:a systematic literature review.Gastrointest Endosc. 2017;85:1169-76.e1. Ishiyama M, Kudo SE, Misawa M, et al. Impact of the clinical use of artificial intelligence-assisted neoplasia detection for colonoscopy:a large-scale prospective, propensity score-matched study (with video).Gastrointest Endosc. 2022;95:155-63. van Rijn JC, Reitsma JB, Stoker J, et al. Polyp miss rate determined by tandem colonoscopy:a systematic review.Am J Gastroenterol. 2006;101:343-50. Turner KO, Genta RM, Sonnenberg A.Lesions of all types exist in colon polyps of all sizes.Am J Gastroenterol. 2018;113:303-6. Livovsky DM, Veikherman D, Golany T, et al. Detection of elusive polyps using a large-scale artificial intelligence system (with videos).Gastrointest Endosc. 2021;94:1099-109. Wang P, Liu P, Glissen Brown JR, et al. Lower adenoma miss rate of computer-aided detection-assisted colonoscopy vs routine white-light colonoscopy in a prospective tandem study.Gastroenterology. 2020;159:1252-61.e5. Glissen Brown JR, Mansour NM, Wang P, et al. Deep learning computer-aided polyp detection reduces adenoma miss rate:a United States Multi-center Randomized Tandem Colonoscopy Study (CADeT-CS Trial).Clin Gastroenterol Hepatol. 2021;S1542-3565(21)00973-3. Lui TKL, Hui CKY, Tsui VWM, et al. New insights on missed colonic lesions dang colonoscopy through artificial intelligence-assisted real-time detection (with video).Gastrointest Endosc. 2021;93:193-200.e1. Li JW, Chia T, Fock KM, et al. Artificial intelligence and polyp detection in colonoscopy:Use of a single neural network to achieve rapid polyp localization for clinical use.J Gastroenterol Hepatol. 2021;36:3298-307. Holzwanger EA, Bilal M, Glissen Brown JR, et al. Benchmarking definitions of false-positive alerts dang computer-aided polyp detection in colonoscopy.Endoscopy. 2021;53:937-40. Li JW, Ang TL.Chiu PWY, Sano Y, Uedo N, Singh R.Narrow-Band Imaging.Endoscopy in Early Gastrointestinal Cancers, Volume 1:Diagnosis. 2021;Singapore Springer Singapore111-9. Kudo S, Tamura S, Nakajima T, et al. Diagnosis of colorectal tumorous lesions by magnifying endoscopy.Gastrointest Endosc. 1996;44:8-14. Kandel P, Wallace MB.Should we resect and discard low risk diminutive colon polyps.Clin Endosc. 2019;52:239-46. von Renteln D, Kaltenbach T, Rastogi A, et al. Simplifying resect and discard strategies for real-time assessment of diminutive colorectal polyps.Clin Gastroenterol Hepatol. 2018;16:706-14. Neumann H, Neumann Sen H, Vieth M, et al. Leaving colorectal polyps in place can be achieved with high accuracy using blue light imaging (BLI).United European Gastroenterol J. 2018;6:1099-105. Rex DK, Kahi C, O'Brien M, et al. The American Society for Gastrointestinal Endoscopy PIVI (Preservation and Incorporation of Valuable Endoscopic Innovations) on real-time endoscopic assessment of the histology of diminutive colorectal polyps.Gastrointest Endosc. 2011;73:419-22. Sano Y, Ikematsu H, Fu KI, et al. Meshed capillary vessels by use of narrow-band imaging for differential diagnosis of small colorectal polyps.Gastrointest Endosc. 2009;69:278-83. Rex DK.Narrow-band imaging without optical magnification for histologic analysis of colorectal polyps.Gastroenterology. 2009;136:1174-81. Sano Y, Tanaka S, Kudo SE, et al. Narrow-band imaging (NBI) magnifying endoscopic classification of colorectal tumors proposed by the Japan NBI Expert Team.Dig Endosc. 2016;28:526-33. Desai M, Kennedy K, Aihara H, et al. External validation of blue light imaging (BLI) criteria for the optical characterization of colorectal polyps by endoscopy experts.J Gastroenterol Hepatol. 2021;36:2728-34. Smith SCL, Siau K, Cannatelli R, et al. Training methods in optical diagnosis and characterization of colorectal polyps:a systematic review and meta-analysis.Endosc Int Open. 2021;9:E716-26. Kobayashi S, Yamada M, Takamaru H, et al. Diagnostic yield of the Japan NBI Expert Team (JNET) classification for endoscopic diagnosis of superficial colorectal neoplasms in a large-scale clinical practice database.United European Gastroenterol J. 2019;7:914-23. Repici A, Ciscato C, Correale L, et al. Narrow-band Imaging International Colorectal Endoscopic Classification to predict polyp histology:REDEFINE study (with videos).Gastrointest Endosc. 2016;84:479-86.e3. Klare P, Haller B, Wormbt S, et al. Narrow-band imaging vs. high definition white light for optical diagnosis of small colorectal polyps:a randomized multicenter trial.Endoscopy. 2016;48:909-15. Byrne MF, Chapados N, Soudan F, et al. Real-time differentiation of adenomatous and hyperplastic diminutive colorectal polyps dang analysis of unaltered videos of standard colonoscopy using a deep learning model.Gut. 2019;68:94-100. Kudo SE, Misawa M, Mori Y, et al. Artificial intelligence-assisted system improves endoscopic identification of colorectal neoplasms.Clin Gastroenterol Hepatol. 2020;18:1874-81.e2. Takeda K, Kudo SE, Mori Y, et al. Accuracy of diagnosing invasive colorectal cancer using computer-aided endocytoscopy.Endoscopy. 2017;49:798-802. Tischendorf JJ, Gross S, Winograd R, et al. Computer-aided classification of colorectal polyps based on vascular patterns:a pilot study.Endoscopy. 2010;42:203-7. Chen PJ, Lin MC, Lai MJ, Lin JC, Lu HH, Tseng et al. Accurate classification of diminutive colorectal polyps using computer-aided analysis.Gastroenterology. 2018;154:568-75. Kominami Y, Yoshida S, Tanaka S, et al. Computer-aided diagnosis of colorectal polyp histology by using a real-time image recognition system and narrow-band imaging magnifying colonoscopy.Gastrointest Endosc. 2016;83:643-9. Song EM, Park B, Ha CA, et al. Endoscopic diagnosis and treatment planning for colorectal polyps using a deep-learning model.Sci Rep. 2020;10:30. Lui TKL, Guo CG, Leung WK.Accuracy of artificial intelligence on histology prediction and detection of colorectal polyps:a systematic review and meta-analysis.Gastrointest Endosc. 2020;92:11-22.e6. Mori Y, Kudo SE, Misawa M, Saito Y, Ikematsu H, Hotta K, et al. Real-time use of artificial intelligence in identification of diminutive polyps dang colonoscopy:a prospective study.Ann Intern Med. 2018;169:357-66. Rodriguez-Diaz E, Baffy G, Lo WK, et al. Real-time artificial intelligence-based histologic classification of colorectal polyps with augmented visualization.Gastrointest Endosc. 2021;93:662-70. Shaukat A, Rector TS, Church TR, et al. Longer withdrawal time is associated with a reduced incidence of interval cancer after screening colonoscopy.Gastroenterology. 2015;149:952-7. Lai EJ, Calderwood AH, Doros G, Fix OK, Jacobson BC.The Boston bowel preparation scale:a valid and reliable instrument for colonoscopy-oriented research.Gastrointest Endosc. 2009;69:3 Pt 2620-5. Taveira F, Hassan C, Kaminski MF, et al. The Colon Endoscopic Bubble Scale (CEBuS):a two-phase evaluation study.Endoscopy. 2022;54:45-51. Coe SG, Panjala C, Heckman MG, et al. Quality in colonoscopy reporting:an assessment of compliance and performance improvement.Dig Liver Dis. 2012;44:660-4. Leyden JE, Doherty GA, Hanley A, et al. Quality of colonoscopy performance among gastroenterology and surgical trainees:a need for common training standards for all trainees?.Endoscopy. 2011;43:935-40. Toyoshima O, Yoshida S, Nishizawa T, et al. Simple feedback of colonoscopy performance improved the number of adenomas per colonoscopy and serrated polyp detection rate.Endosc Int Open. 2021;9:E1032-E8. Gong D, Wu L, Zhang J, et al. Detection of colorectal adenomas with a real-time computer-aided system (ENDOANGEL):a randomised controlled study.Lancet Gastroenterol Hepatol. 2020;5:352-61. Zhou J, Wu L, Wan X, et al. A novel artificial intelligence system for the assessment of bowel preparation (with video).Gastrointest Endosc. 2020;91:428-35.e2. Zhou W, Yao L, Wu H, et al. Multi-step validation of a deep learning-based system for the quantification of bowel preparation:a prospective, observational study.Lancet Digit Health. 2021;3:e697-e706. Yao L, Zhang L, Liu J, et al. Effect of an artificial intelligence-based quality improvement system on efficacy of a computer-aided detection system in colonoscopy:a four-group parallel study.Endoscopy 2021 Nov 25https://doi.org/10.1055/a-1706-6174[Epub ahead of print]. Peterson E, May FP, Kachikian O, et al. Automated identification and assignment of colonoscopy surveillance recommendations for individuals with colorectal polyps.Gastrointest Endosc. 2021;94:978-87. Maeda Y, Kudo SE, Mori Y, et al. Fully automated diagnostic system with artificial intelligence using endocytoscopy to identify the presence of histologic inflammation associated with ulcerative colitis (with video).Gastrointest Endosc. 2019;89:408-15. Stidham RW, Liu W, Bishu S, et al. Performance of a deep learning model vs human reviewers in grading endoscopic disease severity of patients with ulcerative colitis.JAMA Netw Open. 2019;2:e193963. Takenaka K, Ohtsuka K, Fujii T, et al. Development and validation of a deep neural network for accurate evaluation of endoscopic images from patients with ulcerative colitis.Gastroenterology. 2020;158:2150-7. Tanaka S, Kashida H, Saito Y, et al. JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection.Dig Endosc. 2015;27:417-34. Pimentel-Nunes P, Dinis-Ribeiro M, Ponchon T, et al. Endoscopic submucosal dissection:European Society of Gastrointestinal Endoscopy (ESGE) Guideline.Endoscopy. 2015;47:829-54. Li JW, Ang TL, Wang LM, et al. Endoscopic submucosal dissection of colorectal neoplasms:an audit of its safety and efficacy in a single tertiary centre in Singapore.Singapore Med J. 2019;60:526-31. Baxter NN, Virnig DJ, Rothenberger DA, et al. Lymph node evaluation in colorectal cancer patients:a population-based study.J Natl Cancer Inst. 2005;97:219-25. Backes Y, Schwartz MP, Ter Borg F, et al. Multicentre prospective evaluation of real-time optical diagnosis of T1 colorectal cancer in large non-pedunculated colorectal polyps using narrow band imaging (the OPTICAL study).Gut. 2019;68:271-9. Kessels K, Backes Y, Elias SG, et al. Pedunculated morphology of T1 colorectal tumors associates with reduced risk of adverse outcome.Clin Gastroenterol Hepatol. 2019;17:1112-20.e1. Vermeer NCA, Backes Y, Snijders HS, et al. National cohort study on postoperative risks after surgery for submucosal invasive colorectal cancer.BJS Open. 2019;3:210-7. Luo X, Wang J, Han Z, et al. Artificial intelligence-enhanced white-light colonoscopy with attention guidance predicts colorectal cancer invasion depth.Gastrointest Endosc. 2021;94:627-38.e1. Bedrikovetski S, Dudi-Venkata NN, Kroon HM, et al. Artificial intelligence for pre-operative lymph node staging in colorectal cancer:a systematic review and meta-analysis.BMC Cancer. 2021;21:1058. Kudo SE, Ichimasa K, Villard B, et al. Artificial intelligence system to determine risk of T1 colorectal cancer metastasis to lymph node.Gastroenterology. 2021;160:1075-84.e2. Ang TL, East JE.Image-enhanced endoscopy for detection and diagnosis of colonic neoplasia:Time to shift focus.J Gastroenterol Hepatol. 2021;36:2635-6. Spadaccini M, Iannone A, Maselli R, et al. Computer-aided detection versus advanced imaging for detection of colorectal neoplasia:a systematic review and network meta-analysis.Lancet Gastroenterol Hepatol. 2021;6:793-802.
2. Kaminski MF, Thomas-Gibson S, Bugajski M, et al. Performance measures for lower gastrointestinal endoscopy: a European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative. Endoscopy 2017; 49:378-97. https://doi.org/10.1055/s-0043-103411
PMid:28268235
3. Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy. Gastrointest Endosc 2015; 81:31-53. https://doi.org/10.1016/j.gie.2014.07.058
PMid:25480100
4. Corley DA, Levin TR, Doubeni CA. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med 2014; 370:2541. https://doi.org/10.1056/NEJMoa1309086
PMCid:PMC4036494
5. Kaltenbach T, Anderson JC, Burke CA, et al. Endoscopic removal of colorectal lesions-recommendations by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2020; 158:1095-1129. https://doi.org/10.1053/j.gastro.2019.12.018
PMid:32122632
7. Gupta S, Lieberman D, Anderson JC, et al. Recommendations for follow-up after colonoscopy and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc 2020; 91:463-85.e5. https://doi.org/10.1016/j.gie.2020.01.014
PMid:32044106 PMCid:PMC7389642
8. Hassan C, Antonelli G, Dumonceau JM, et al. Post-polypectomy colonoscopy surveillance: European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Update 2020. Endoscopy 2020; 52:687-700. https://doi.org/10.1055/a-1185-3109
PMid:32572858
9. Shalev-Shwartz S. Understanding Machine Learning: from Theory to Algorithms. New York: Cambridge University Press, 2014. https://doi.org/10.1017/CBO9781107298019
10. Kaul V, Enslin S, Gross SA. History of artificial intelligence in medicine. Gastrointest Endosc 2020; 92:807-12. https://doi.org/10.1016/j.gie.2020.06.040
PMid:32565184
11. Li JW, Ang TL. Colonoscopy and artificial intelligence: Bridging the gap or a gap needing to be bridged? Artif Intell Gastrointest Endosc 2021; 2:36-49. https://doi.org/10.37126/aige.v2.i2.36
12. Chen H, Sung JJY. Potentials of AI in medical image analysis in Gastroenterology and Hepatology. J Gastroenterol Hepatol 2021; 36:31-8. https://doi.org/10.1111/jgh.15327
PMid:33140875
13. Ahmad OF, Mori Y, Misawa M, et al. Establishing key research questions for the implementation of artificial intelligence in colonoscopy: a modified Delphi method. Endoscopy 2021; 53:893-901. https://doi.org/10.1055/a-1306-7590
PMid:33167043 PMCid:PMC8390295
14. Berzin TM, Parasa S, Wallace MB, et al. Position statement on priorities for artificial intelligence in GI endoscopy: a report by the ASGE Task Force. Gastrointest Endosc 2020; 92:951-9. https://doi.org/10.1016/j.gie.2020.06.035
PMid:32565188
15. Bisschops R, East JE, Hassan C, et al. Advanced imaging for detection and differentiation of colorectal neoplasia: European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Update 2019. Endoscopy 2019; 51:1155-79. https://doi.org/10.1055/a-1031-7657
PMid:31711241
16. Pohl H, Robertson DJ. Colorectal cancers detected after colonoscopy frequently result from missed lesions. Clin Gastroenterol Hepatol 2010; 8:858-64. https://doi.org/10.1016/j.cgh.2010.06.028
PMid:20655393
17. Robertson DJ, Lieberman DA, Winawer SJ, et al. Colorectal cancers soon after colonoscopy: a pooled multicohort analysis. Gut 2014; 63:949-56. https://doi.org/10.1136/gutjnl-2012-303796
PMid:23793224 PMCid:PMC4383397
18. Anderson R, Burr NE, Valori R. Causes of post-colonoscopy colorectal cancers based on World Endoscopy Organization System of Analysis. Gastroenterology 2020; 158:1287-99.e2. https://doi.org/10.1053/j.gastro.2019.12.031
PMid:31926170
19. Zhao S, Wang S, Pan P, et al. Magnitude, risk factors, and factors associated with adenoma miss rate of tandem colonoscopy: a systematic review and metaanalysis. Gastroenterology 2019; 156:1661-74.e11. https://doi.org/10.1053/j.gastro.2019.01.260
PMid:30738046
20. Rex DK, Cutler CS, Lemmel GT, et al. Colonoscopic miss rates of adenomas determined by back-to-back colonoscopies. Gastroenterology 1997; 112:24-8. https://doi.org/10.1016/S0016-5085(97)70214-2
21. Leufkens AM, van Oijen MGH, Vleggaar FP, Siersema PD. Factors influencing the miss rate of polyps in a back-to-back colonoscopy study. Endoscopy 2012; 44:470-5. https://doi.org/10.1055/s-0031-1291666
PMid:22441756
22. Lee CK, Park DI, Lee SH, et al. Participation by experienced endoscopy nurses increases the detection rate of colon polyps during a screening colonoscopy: a multicenter, prospective, randomized study. Gastrointest Endosc 2011; 74:1094-102. https://doi.org/10.1016/j.gie.2011.06.033
PMid:21889137
23. Buchner AM, Shahid MW, Heckman MG, et al. Trainee participation is associated with increased small adenoma detection. Gastrointest Endosc 2011; 73:1223-31. https://doi.org/10.1016/j.gie.2011.01.060
PMid:21481861
24. Hassan C, Spadaccini M, Iannone A, et al. Performance of artificial intelligence in colonoscopy for adenoma and polyp detection: a systematic review and meta-analysis. Gastrointest Endosc 2021; 93:77-85.e6. https://doi.org/10.1016/j.gie.2020.06.059
PMid:32598963
25. Wang P, Berzin TM, Glissen Brown JR, et al. Real-time automatic detection system increases colonoscopic polyp and adenoma detection rates: a prospective randomised controlled study. Gut 2019; 68:1813-9. https://doi.org/10.1136/gutjnl-2018-317500
PMid:30814121 PMCid:PMC6839720
26. Wang P, Liu X, Berzin TM, et al. Effect of a deep-learning computer-aided detection system on adenoma detection during colonoscopy (CADe-DB trial): a double-blind randomised study. Lancet Gastroenterol Hepatol 2020; 5:343-51. https://doi.org/10.1016/S2468-1253(19)30411-X
27. Repici A, Badalamenti M, Maselli R, et al. Efficacy of real-time computer-aided detection of colorectal neoplasia in a randomized trial. Gastroenterology 2020; 159:512-20.e7. https://doi.org/10.1053/j.gastro.2020.04.062
PMid:32371116
28. Su JR, Li Z, Shao XJ, et al. Impact of a real-time automatic quality control system on colorectal polyp and adenoma detection: a prospective randomized controlled study (with videos). Gastrointest Endosc 2020; 91:415-24.e4. https://doi.org/10.1016/j.gie.2019.08.026
PMid:31454493
29. Liu WN, Zhang YY, Bian XQ, et al. Study on detection rate of polyps and adenomas in artificial-intelligence-aided colonoscopy. Saudi J Gastroenterol 2020; 26:13-9. https://doi.org/10.4103/sjg.SJG_377_19
PMid:31898644 PMCid:PMC7045775
30. Vleugels JLA, Hazewinkel Y, Fockens P, Dekker E. Natural history of diminutive and small colorectal polyps: a systematic literature review. Gastrointest Endosc 2017; 85:1169-76.e1. https://doi.org/10.1016/j.gie.2016.12.014
PMid:28024986
31. Ishiyama M, Kudo SE, Misawa M, et al. Impact of the clinical use of artificial intelligence-assisted neoplasia detection for colonoscopy: a large-scale prospective, propensity score-matched study (with video). Gastrointest Endosc 2022; 95:155-63. https://doi.org/10.1016/j.gie.2021.07.022
PMid:34352255
32. van Rijn JC, Reitsma JB, Stoker J, et al. Polyp miss rate determined by tandem colonoscopy: a systematic review. Am J Gastroenterol 2006; 101:343-50. https://doi.org/10.1111/j.1572-0241.2006.00390.x
PMid:16454841
33. Turner KO, Genta RM, Sonnenberg A. Lesions of all types exist in colon polyps of all sizes. Am J Gastroenterol 2018; 113:303-6. https://doi.org/10.1038/ajg.2017.439
PMid:29231190
34. Livovsky DM, Veikherman D, Golany T, et al. Detection of elusive polyps using a large-scale artificial intelligence system (with videos). Gastrointest Endosc 2021; 94:1099-109. https://doi.org/10.1016/j.gie.2021.06.021
PMid:34216598
35. Wang P, Liu P, Glissen Brown JR, et al. Lower adenoma miss rate of computer-aided detection-assisted colonoscopy vs routine white-light colonoscopy in a prospective tandem study. Gastroenterology 2020; 159:1252-61.e5. https://doi.org/10.1053/j.gastro.2020.06.023
PMid:32562721
36. Glissen Brown JR, Mansour NM, Wang P, et al. Deep learning computer-aided polyp detection reduces adenoma miss rate: a United States Multi-center Randomized Tandem Colonoscopy Study (CADeT-CS Trial). Clin Gastroenterol Hepatol 2021; S1542-3565(21)00973-3.
37. Lui TKL, Hui CKY, Tsui VWM, et al. New insights on missed colonic lesions during colonoscopy through artificial intelligence-assisted real-time detection (with video). Gastrointest Endosc 2021; 93:193-200.e1. https://doi.org/10.1016/j.gie.2020.04.066
PMid:32376335
38. Li JW, Chia T, Fock KM, et al. Artificial intelligence and polyp detection in colonoscopy: Use of a single neural network to achieve rapid polyp localization for clinical use. J Gastroenterol Hepatol 2021; 36:3298-307. https://doi.org/10.1111/jgh.15642
PMid:34327729
39. Holzwanger EA, Bilal M, Glissen Brown JR, et al. Benchmarking definitions of false-positive alerts during computer-aided polyp detection in colonoscopy. Endoscopy 2021; 53:937-40. https://doi.org/10.1055/a-1302-2942
PMid:33137833
40. Li JW, Ang TL. Narrow-Band Imaging. In: Chiu PWY, Sano Y, Uedo N, Singh R, eds. Endoscopy in Early Gastrointestinal Cancers, Volume 1: Diagnosis. Singapore: Springer Singapore, 2021: 111-9. https://doi.org/10.1007/978-981-10-6769-3_13
41. Kudo S, Tamura S, Nakajima T, et al. Diagnosis of colorectal tumorous lesions by magnifying endoscopy. Gastrointest Endosc 1996; 44:8-14. https://doi.org/10.1016/S0016-5107(96)70222-5
42. Kandel P, Wallace MB. Should we resect and discard low risk diminutive colon polyps. Clin Endosc 2019; 52:239-46. https://doi.org/10.5946/ce.2018.136
PMid:30661337 PMCid:PMC6547333
43. von Renteln D, Kaltenbach T, Rastogi A, et al. Simplifying resect and discard strategies for real-time assessment of diminutive colorectal polyps. Clin Gastroenterol Hepatol 2018; 16:706-14. https://doi.org/10.1016/j.cgh.2017.11.036
PMid:29174789
44. Neumann H, Neumann Sen H, Vieth M, et al. Leaving colorectal polyps in place can be achieved with high accuracy using blue light imaging (BLI). United European Gastroenterol J 2018; 6:1099-105. https://doi.org/10.1177/2050640618769731
PMid:30228899 PMCid:PMC6137600
45. Rex DK, Kahi C, O'Brien M, et al. The American Society for Gastrointestinal Endoscopy PIVI (Preservation and Incorporation of Valuable Endoscopic Innovations) on real-time endoscopic assessment of the histology of diminutive colorectal polyps. Gastrointest Endosc 2011; 73:419-22. https://doi.org/10.1016/j.gie.2011.01.023
PMid:21353837
46. Sano Y, Ikematsu H, Fu KI, et al. Meshed capillary vessels by use of narrow-band imaging for differential diagnosis of small colorectal polyps. Gastrointest Endosc 2009; 69:278-83. https://doi.org/10.1016/j.gie.2008.04.066
PMid:18951131
47. Rex DK. Narrow-band imaging without optical magnification for histologic analysis of colorectal polyps. Gastroenterology 2009; 136:1174-81. https://doi.org/10.1053/j.gastro.2008.12.009
PMid:19187781
48. Sano Y, Tanaka S, Kudo SE, et al. Narrow-band imaging (NBI) magnifying endoscopic classification of colorectal tumors proposed by the Japan NBI Expert Team. Dig Endosc 2016; 28:526-33. https://doi.org/10.1111/den.12644
PMid:26927367
49. Desai M, Kennedy K, Aihara H, et al. External validation of blue light imaging (BLI) criteria for the optical characterization of colorectal polyps by endoscopy experts. J Gastroenterol Hepatol 2021; 36:2728-34. https://doi.org/10.1111/jgh.15529
PMid:33928679
50. Smith SCL, Siau K, Cannatelli R, et al. Training methods in optical diagnosis and characterization of colorectal polyps: a systematic review and meta-analysis. Endosc Int Open 2021; 9:E716-26. https://doi.org/10.1055/a-1381-7181
PMid:33937513 PMCid:PMC8062231
51. Kobayashi S, Yamada M, Takamaru H, et al. Diagnostic yield of the Japan NBI Expert Team (JNET) classification for endoscopic diagnosis of superficial colorectal neoplasmsin a large-scale clinical practice database. United European Gastroenterol J 2019; 7:914-23. https://doi.org/10.1177/2050640619845987
PMid:31428416 PMCid:PMC6683640
52. Repici A, Ciscato C, Correale L, et al. Narrow-band Imaging International Colorectal Endoscopic Classification to predict polyp histology: REDEFINE study (with videos). Gastrointest Endosc 2016; 84:479-86.e3. https://doi.org/10.1016/j.gie.2016.02.020
PMid:26928372
53. Klare P, Haller B, Wormbt S, et al. Narrow-band imaging vs. high definition white light for optical diagnosis of small colorectal polyps: a randomized multicenter trial. Endoscopy 2016; 48:909-15. https://doi.org/10.1055/s-0042-110650
PMid:27448051
54. Byrne MF, Chapados N, Soudan F, et al. Real-time differentiation of adenomatous and hyperplastic diminutive colorectal polyps during analysis of unaltered videos of standard colonoscopy using a deep learning model. Gut 2019; 68:94-100. https://doi.org/10.1136/gutjnl-2017-314547
PMid:29066576 PMCid:PMC6839831
55. Kudo SE, Misawa M, Mori Y, et al. Artificial intelligence-assisted system improves endoscopic identification of colorectal neoplasms. Clin Gastroenterol Hepatol 2020; 18:1874-81.e2. https://doi.org/10.1016/j.cgh.2019.09.009
PMid:31525512
56. Takeda K, Kudo SE, Mori Y, et al. Accuracy of diagnosing invasive colorectal cancer using computer-aided endocytoscopy. Endoscopy 2017; 49:798-802. https://doi.org/10.1055/s-0043-105486
PMid:28472832
57. Tischendorf JJ, Gross S, Winograd R, et al. Computer-aided classification of colorectal polyps based on vascular patterns: a pilot study. Endoscopy 2010; 42:203-7. https://doi.org/10.1055/s-0029-1243861
PMid:20101564
58. Chen PJ, Lin MC, Lai MJ, Lin JC, Lu HH, Tseng et al. Accurate classification of diminutive colorectal polyps using computer-aided analysis. Gastroenterology 2018; 154:568-75. https://doi.org/10.1053/j.gastro.2017.10.010
PMid:29042219
59. Kominami Y, Yoshida S, Tanaka S, et al. Computer-aided diagnosis of colorectal polyp histology by using a real-time image recognition system and narrow-band imaging magnifying colonoscopy. Gastrointest Endosc 2016; 83:643-9. https://doi.org/10.1016/j.gie.2015.08.004
PMid:26264431
60. Song EM, Park B, Ha CA, et al. Endoscopic diagnosis and treatment planning for colorectal polyps using a deep-learning model. Sci Rep 2020; 10:30. https://doi.org/10.1038/s41598-019-56697-0
PMid:31913337 PMCid:PMC6949236
61. Lui TKL, Guo CG, Leung WK. Accuracy of artificial intelligence on histology prediction and detection of colorectal polyps: a systematic review and metaanalysis. Gastrointest Endosc 2020; 92:11-22.e6. https://doi.org/10.1016/j.gie.2020.02.033
PMid:32119938
62. Mori Y, Kudo SE, Misawa M, Saito Y, Ikematsu H, Hotta K, et al. Real-time use of artificial intelligence in identification of diminutive polyps during colonoscopy: a prospective study. Ann Intern Med 2018; 169:357-66. https://doi.org/10.7326/M18-0249
PMid:30105375
63. Rodriguez-Diaz E, Baffy G, Lo WK, et al. Real-time artificial intelligence-based histologic classification of colorectal polyps with augmented visualization. Gastrointest Endosc 2021; 93:662-70. https://doi.org/10.1016/j.gie.2020.09.018
PMid:32949567
64. Shaukat A, Rector TS, Church TR, et al. Longer withdrawal time is associated with a reduced incidence of interval cancer after screening colonoscopy. Gastroenterology 2015; 149:952-7. https://doi.org/10.1053/j.gastro.2015.06.044
PMid:26164494
65. Lai EJ, Calderwood AH, Doros G, Fix OK, Jacobson BC. The Boston bowel preparation scale: a valid and reliable instrument for colonoscopy-oriented research. Gastrointest Endosc 2009; 69(3 Pt 2):620-5. https://doi.org/10.1016/j.gie.2008.05.057
PMid:19136102 PMCid:PMC2763922
66. Taveira F, Hassan C, Kaminski MF, et al. The Colon Endoscopic Bubble Scale (CEBuS): a two-phase evaluation study. Endoscopy 2022; 54:45-51. https://doi.org/10.1055/a-1331-4325
PMid:33285583
67. Coe SG, Panjala C, Heckman MG, et al. Quality in colonoscopy reporting: an assessment of compliance and performance improvement. Dig Liver Dis 2012; 44:660-4. https://doi.org/10.1016/j.dld.2012.03.022
PMid:22579446
68. Leyden JE, Doherty GA, Hanley A, et al. Quality of colonoscopy performance among gastroenterology and surgical trainees: a need for common training standards for all trainees? Endoscopy 2011; 43:935-40. https://doi.org/10.1055/s-0030-1256633
PMid:21997723
69. Toyoshima O, Yoshida S, Nishizawa T, et al. Simple feedback of colonoscopy performance improved the number of adenomas per colonoscopy and serrated polyp detection rate. Endosc Int Open 2021; 9:E1032-E8. https://doi.org/10.1055/a-1393-5469
PMid:34222627 PMCid:PMC8211485
70. Gong D, Wu L, Zhang J, et al. Detection of colorectal adenomas with a realtime computer-aided system (ENDOANGEL): a randomised controlled study. Lancet Gastroenterol Hepatol 2020; 5:352-61. https://doi.org/10.1016/S2468-1253(19)30413-3
71. Zhou J, Wu L, Wan X, et al. A novel artificial intelligence system for the assessment of bowel preparation (with video). Gastrointest Endosc 2020; 91:428-35.e2. https://doi.org/10.1016/j.gie.2019.11.026
PMid:31783029
72. Zhou W, Yao L, Wu H, et al. Multi-step validation of a deep learning-based system for the quantification of bowel preparation: a prospective, observational study. Lancet Digit Health 2021; 3:e697-e706. https://doi.org/10.1016/S2589-7500(21)00109-6
73. Yao L, Zhang L, Liu J, et al. Effect of an artificial intelligence-based quality improvement system on efficacy of a computer-aided detection system in colonoscopy: a four-group parallel study. Endoscopy 2021 Nov 25. https://doi.org/10.1055/a-1706-6174. [Epub ahead of print] https://doi.org/10.1055/a-1706-6174
74. Peterson E, May FP, Kachikian O, et al. Automated identification and assignment of colonoscopy surveillance recommendations for individuals with colorectal polyps. Gastrointest Endosc 2021; 94:978-87. https://doi.org/10.1016/j.gie.2021.05.036
PMid:34087201
75. Maeda Y, Kudo SE, Mori Y, et al. Fully automated diagnostic system with artificial intelligence using endocytoscopy to identify the presence of histologic inflammation associated with ulcerative colitis (with video). Gastrointest Endosc 2019; 89:408-15. https://doi.org/10.1016/j.gie.2018.09.024
PMid:30268542
76. Stidham RW, Liu W, Bishu S, et al. Performance of a deep learning model vs human reviewers in grading endoscopic disease severity of patients with ulcerative colitis. JAMA Netw Open 2019; 2:e193963. https://doi.org/10.1001/jamanetworkopen.2019.3963
PMid:31099869 PMCid:PMC6537821
77. Takenaka K, Ohtsuka K, Fujii T, et al. Development and validation of a deep neural network for accurate evaluation of endoscopic images from patients with ulcerative colitis. Gastroenterology 2020; 158:2150-7. https://doi.org/10.1053/j.gastro.2020.02.012
PMid:32060000
78. Tanaka S, Kashida H, Saito Y, et al. JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig Endosc 2015; 27:417-34. https://doi.org/10.1111/den.12456
PMid:25652022
79. Pimentel-Nunes P, Dinis-Ribeiro M, Ponchon T, et al. Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2015; 47:829-54. https://doi.org/10.1055/s-0034-1392882
PMid:26317585
80. Li JW, Ang TL, Wang LM, et al. Endoscopic submucosal dissection of colorectal neoplasms: an audit of its safety and efficacy in a single tertiary centre in Singapore. Singapore Med J 2019; 60:526-31. https://doi.org/10.11622/smedj.2019022
PMid:30773601 PMCid:PMC6875819
81. Baxter NN, Virnig DJ, Rothenberger DA, et al. Lymph node evaluation in colorectal cancer patients: a population-based study. J Natl Cancer Inst 2005; 97:219-25. https://doi.org/10.1093/jnci/dji020
PMid:15687365
82. Backes Y, Schwartz MP, Ter Borg F, et al. Multicentre prospective evaluation of real-time optical diagnosis of T1 colorectal cancer in large non-pedunculated colorectal polyps using narrow band imaging (the OPTICAL study). Gut 2019; 68:271-9. https://doi.org/10.1136/gutjnl-2017-314723
PMid:29298873
83. Kessels K, Backes Y, Elias SG, et al. Pedunculated morphology of T1 colorectal tumors associates with reduced risk of adverse outcome. Clin Gastroenterol Hepatol 2019; 17:1112-20.e1. https://doi.org/10.1016/j.cgh.2018.08.041
PMid:30130623
84. Vermeer NCA, Backes Y, Snijders HS, et al. National cohort study on postoperative risks after surgery for submucosal invasive colorectal cancer. BJS Open 2019; 3:210-7. https://doi.org/10.1002/bjs5.50125
PMid:30957069 PMCid:PMC6433330
85. Luo X, Wang J, Han Z, et al. Artificial intelligence-enhanced white-light colonoscopy with attention guidance predicts colorectal cancer invasion depth. Gastrointest Endosc 2021; 94:627-38.e1. https://doi.org/10.1016/j.gie.2021.03.936
PMid:33852902
86. Bedrikovetski S, Dudi-Venkata NN, Kroon HM, et al. Artificial intelligence for pre-operative lymph node staging in colorectal cancer: a systematic review and meta-analysis. BMC Cancer 2021; 21:1058. https://doi.org/10.1186/s12885-021-08773-w
PMid:34565338 PMCid:PMC8474828
87. Kudo SE, Ichimasa K, Villard B, et al. Artificial intelligence system to determine risk of T1 colorectal cancer metastasis to lymph node. Gastroenterology 2021; 160:1075-84.e2. https://doi.org/10.1053/j.gastro.2020.09.027
PMid:32979355
88. Ang TL, East JE. Image-enhanced endoscopy for detection and diagnosis of colonic neoplasia: Time to shift focus. J Gastroenterol Hepatol 2021; 36:2635-6. https://doi.org/10.1111/jgh.15684
PMid:34622988
89. Spadaccini M, Iannone A, Maselli R, et al. Computer-aided detection versus advanced imaging for detection of colorectal neoplasia: a systematic review and network meta-analysis. Lancet Gastroenterol Hepatol 2021; 6:793-802. https://doi.org/10.1016/S2468-1253(21)00215-6