Author Information >Copyright and License information >
1Department of Cardiology, National University Heart Centre Singapore, Singapore 2Yong Loo Lin School of Medicine, National University of Singapore, Singapore Correspondence: Dr Joshua Ping-Yun Loh, Assistant Professor, Department of Cardiology, National University Heart Centre Singapore, 1E Kent Ridge Road, NUHS Tower Block Level 9, Singapore 119228. joshua_py_loh@nuhs.edu.sg
Stress (Takotsubo) cardiomyopathy (SC) is a cardiomyopathy characterised by transient myocardial dysfunction, commonly triggered by a surge in catecholamine. Electrocardiographic features may mimic other conditions, such as myocardial infarction. We presented two cases of SC and reviewed the electrocardiographic features of this disease entity.
Keywords: electrocardiography, stress cardiomyopathy, ST elevation, Takotsubo, T wave inversion
CASE 1 CLINICAL PRESENTATION
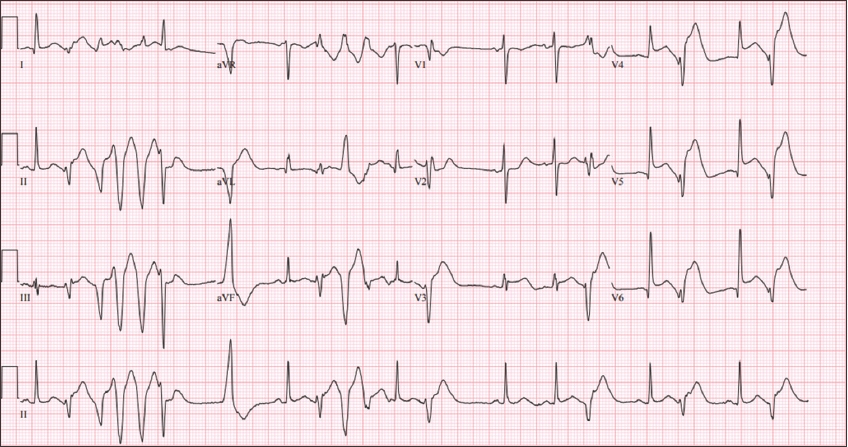
A 64-year-old woman presented with central crushing chest pain associated with acute nausea, diaphoresis and palpitations on Postoperative Day 2 of a right total knee replacement surgery. She had a background history of diabetes mellitus and dyslipidaemia. Physical examination revealed a soft systolic murmur and an oxygen saturation of 90% on room air. What does her electrocardiogram (ECG) show (Fig. 1)?
Fig. 1
Case 1: ECG of a 64-year-old woman who presented with central crushing chest pain.
ECG INTERPRETATION
ECG shows ST elevation in leads V3–V6. Frequent premature ventricular contractions (PVCs), couplets and salvos of PVCs are seen. There is ST segment depression in aVR and V1. The ST segment in V2 is not elevated.
CLINICAL COURSE
Urgent cardiac catheterisation was performed in view of ongoing chest pain and ST elevation. Coronary angiography showed normal coronary arteries. In view of her hypoxia, computed tomographic pulmonary angiography was performed, which did not demonstrate any pulmonary embolism. Urgent transthoracic echocardiography showed an ejection fraction of 10% with akinesia at the apex and increased myocardial contraction at the base. The patient subsequently developed cardiogenic shock with multiorgan failure and required venoarterial extracorporeal membrane oxygenation (ECMO) as well as renal replacement therapy. The peak troponin I value was 42,151 ng/L (reference: 0–39 ng/L). ECMO was stopped on the fourth day. The patient subsequently improved clinically and was discharged after a prolonged stay. The patient was treated with bisoprolol. Repeat transthoracic echocardiography four months later showed resolution of the wall motion abnormalities and an ejection fraction of 60%.
CASE 2 CLINICAL PRESENTATION
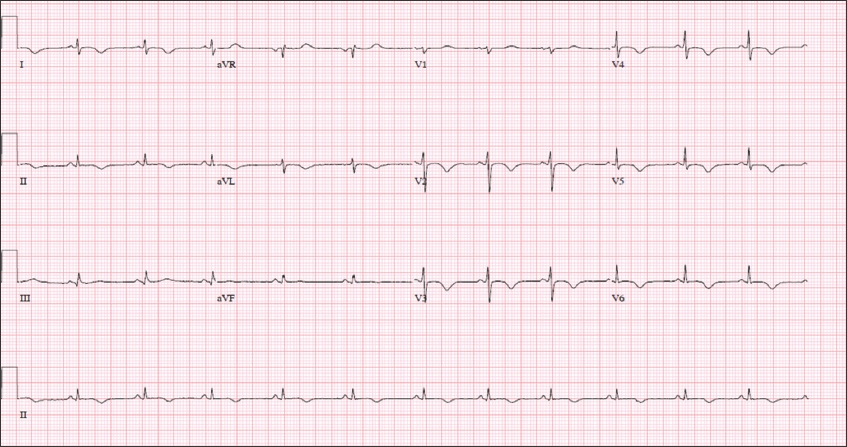
A 35-year-old woman with no significant past medical history was undergoing an elective left hemithyroidectomy for a left thyroid nodule. After anaesthetic induction and upon skin incision, the patient became hypotensive and bradycardic with development of complete heart block (seen on the cardiac monitor). What does the ECG show (Fig. 2)?
Fig. 2
Case 2: ECG of a 35-year-old woman undergoing an elective left hemithyroidectomy for a left thyroid nodule.
ECG INTERPRETATION
The ECG shows widespread T wave inversion in leads V2–V6, I and aVL, as well as in lead II. The ECG is also low voltage (QRS amplitude < 5 mm in the limb leads and < 10 mm in the precordial leads).
CLINICAL COURSE
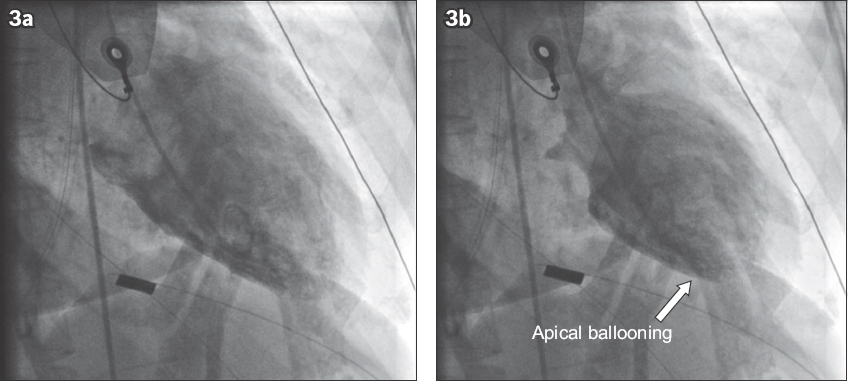
In view of her cardiogenic shock, an urgent cardiac catheterisation was performed, which demonstrated normal coronary arteries. Left ventriculography showed the presence of a typical apical ballooning pattern of stress cardiomyopathy (Fig. 3). Her peak troponin I level was 5,380 ng/L (reference: 0–39 ng/L). Transthoracic echocardiography showed apical akinesia with the base being relatively unaffected and an ejection fraction of 30%. The patient was treated with lisinopril. Serum and urinary metanephrine levels were normal. Repeat transthoracic echocardiography performed two months after discharge showed resolution of akinesia and no regional wall motion abnormalities, with recovery of ejection fraction to 65%.
Fig. 3
(a) Diastolic and (b) systolic left ventriculograms show apical to mid-ventricular ballooning with basal hyperkinesis.
DISCUSSION
Stress (Takotsubo) cardiomyopathy (SC) is a rare cardiomyopathy typically characterised by transient myocardial dysfunction of the apical or mid-ventricular segments of the left ventricle in the absence of an obstructive coronary anatomy, secondary to a catecholamine surge. The condition is usually self-limiting.(1) The Mayo Clinic diagnostic criteria has been proposed, based on expert consensus, to diagnose the condition and one of the criteria describes new ECG abnormalities (specifically referring to either T wave inversions or ST segment elevations).(1) In stable patients, cardiac magnetic resonance imaging may help to distinguish SC from myocarditis and myocardial infarction, as this imaging modality is able to demonstrate scars and late gadolinium enhancement. In the rest of this paper, we review the literature on the possible ECG manifestations of SC and highlight the myriad of ECG presentations beyond the current existing diagnostic criteria.
Q waves
SC has been associated with a finding of transient or persistent Q wave formation.(1)
QRS complexes
Studies have described QRS complexes in SC that show low voltages and attenuation of the amplitude of QRS complexes (as in Case 2) in serial ECGs due to myocardial oedema, with a corresponding shortening of the QRS duration.(1,2)
ST segment
ST elevation in −aVR (i.e. ST depression in aVR) with various permutations of ST elevation and T wave inversions are characteristic of SC.(3) It is of particular interest that ST elevation seldom affects V1, as the akinetic segments are situated away from the V1 lead.(4)
T waves
SC patients have diffuse T wave inversions extending throughout multiple leads, and the depth of the inversions correlates with the magnitude of myocardial oedema.(4) A positive T wave in aVR and a lack of negative T wave in V1 are highly sensitive and specific for SC.(1) Rarer T wave manifestations have also been reported. A Wellens’ syndrome-type ECG pattern with biphasic T waves has previously been reported and has been attributed to a gradient of myocardial oedema on the left ventricle seen on cardiac magnetic resonance imaging.(5)
QT interval
SC has been associated with abnormalities in ventricular repolarisation, causing a prolongation of the QT interval, and is a known cause of acquired long QT syndrome.(1) QT dispersion and Tpeak-to-Tend are also increased. Reversal of all the above intervals in the chronic phase has been reported.(6)
Arrhythmias
SC patients may present with a variety of tachyarrhythmia and bradyarrhythmia. Tachycardias include atrial fibrillation as well as more serious rhythms such as torsades de pointes (in association with the prolongation of QTc), polymorphic ventricular tachycardia and ventricular fibrillation.(7-10) Bradycardias include conduction blocks of various degrees.(11)
Other ECG presentations
SC may present as a new-onset left bundle branch block mimicking ST elevation myocardial infarction, and this has been reported in up to 9% of patients in one study.(12)
Studies comparing SC with other conditions
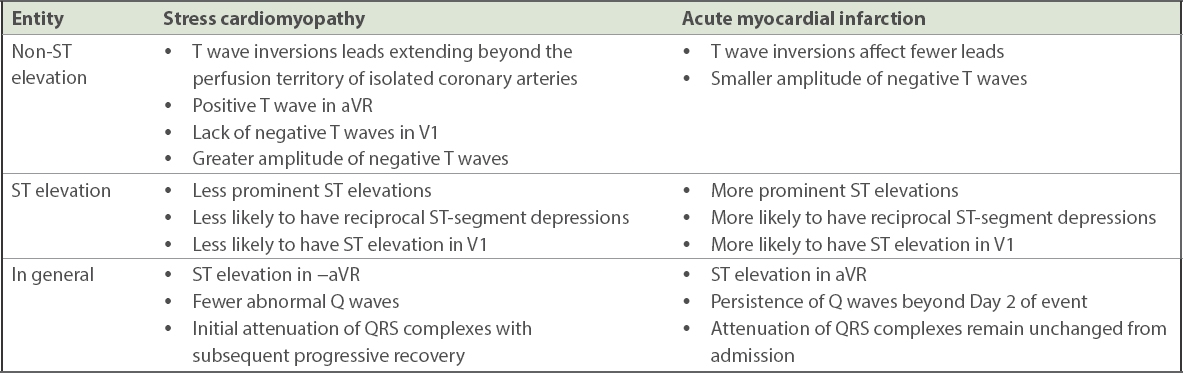
Differentiating SC from other conditions, in particular acute myocardial infarction (AMI), is of interest because of the potential implications on therapy upon presentation.(13) A summary of the reported ECG differences between SC and AMI are presented in Table I.(1,4,9,14-17) The ECGs of SC and AMI patients are subdivided into those with ST elevations and those without. It is worth noting that several studies have disputed the use of ECG criteria to differentiate between SC and AMI.(17)
Table I
Reported electrocardiographic differences between stress cardiomyopathy and acute myocardial infarction.
Interestingly, the ECG changes of SC may resemble those of acute pericarditis, with more diffuse ST segment elevations, concave ST segment elevations and depressed PR segments.(18) It is postulated that this possibly reflects acute circumferential subepicardial ischaemia in SC.(18)
ECG markers of prognosis
Longer QT intervals are associated with poorer outcomes. These patients are more likely to present with dyspnoea and to have higher levels of N-terminal pro B-type natriuretic peptide. They are also more likely than those with a normal QT interval to require re-hospitalisation, mechanical ventilation and vasopressors for shock, as well as develop arrhythmias and die.(19) Prolonged QRS duration is also associated with higher in-hospital mortality, cardiac death, ventilator use, ventricular arrhythmias and circulatory failure.(20) Other reported adverse prognostic markers include a higher heart rate and larger sum of ST elevations in all 12 leads.(21) Persistent Q waves are a poor prognostic marker.(4) There are no reported differences in clinical complications in patients presenting with ST or non-ST elevation ECGs in SC.(22)
Other considerations
The ECG manifestations of SC could vary depending on the type of SC. The apical or combined apical and mid-ventricular variants have been associated with ST elevations, while the mid-ventricular variants alone have been associated with T wave inversions.(22) ECG changes more often affect all leads in apical variants, while only leads V2 and V3 are affected in the mid-ventricular variants.(23) SC can coexist with other pathologies (e.g. acute pericarditis), complicating ECG interpretation.(24) Ethnic differences in ECG presentations have also been described, with Asian patients having more ST segment elevations as compared to Caucasians.(25) However, there has not been any reported ECG differences between male and female patients.(22)
CONCLUSION
This paper discussed two cases of SC with ECG manifestations. It also described the reported ECG manifestations of SC. Practitioners should take note of these clinical presentations to heighten their suspicion so as to successfully diagnose this cardiomyopathy.
References Duran-Cambra A, Sutil-Vega M, Fiol M, et al. Systematic review of the electrocardiographic changes in the Takotsubo syndrome.Ann Noninvasive Electrocardiol. 2015;20:1-6. Madias JE, Macfarlane PW.Artificial attenuation of ECG voltage produces shortening of the corresponding QRS duration: clinical implications for patients with edema.Pacing Clin Electrophysiol. 2005;28:1060-5. Frangieh AH, Obeid S, Ghadri JR, et al. Inter TAK Collaborators. ECG criteria to differentiate between takotsubo (stress) cardiomyopathy and myocardial infarction.J Am Heart Assoc. 2016;5:e003418. Thakar S, Chandra P, Hollander G, Lichstein E.Electrocardiographic changes in Takotsubo cardiomyopathy.Pacing Clin Electrophysiol. 2011;34:1278-82. Perazzolo Marra M, Zorzi A, Corbetti F, et al. Apicobasal gradient of left ventricular myocardial edema underlies transient T-wave inversion and QT interval prolongation (Wellens'ECG pattern) in Tako-Tsubo cardiomyopathy.Heart Rhythm. 2013;10:70-7. Mugnai G, Vassanelli F, Pasqualin G, et al. Dynamic changes of repolarization abnormalities in takotsubo cardiomyopathy.Acta Cardiol. 2015;70:225-32. Hasdemir C, Vuran O, Yuksel A, Yavuzgil O.Stress cardiomyopathy (Tako-Tsubo) associated with sustained polymorphic ventricular tachycardia.Pacing Clin Electrophysiol. 2013;36:e111-4. Madias J.A patient with ventricular fibrillation and inverted Takotsubo syndrome triggered by sinus surgery: plausible causes, and electrocardiographic features.Turk Kardiyol Dern Ars. 2016;44:535. Namgung J.Electrocardiographic findings in Takotsubo cardiomyopathy: ECG evolution and its difference from the ECG of acute coronary syndrome.Clin Med Insights Cardiol. 2014;8:29-34. Valbusa A, Ingrassia S, Rosa GM, et al. Takotsubo cardiomyopathy and torsade de pointes in myasthenic crisis: be aware of QT prolongation.Am J Emerg Med. 2013;31:1717-8. Cativo EH, Valvani R, Mene-Afejuku TO, Cativo DP, Mushiyev S.A rare association of Takotsubo cardiomyopathy with high-degree atrioventricular block.Case Rep Cardiol. 2017;2017:6989438. Parodi G, Salvadori C, Del Pace S, et al. Tuscany Registry of Tako-Tsubo Cardiomyopathy. Left bundle branch block as an electrocardiographic pattern at presentation of patients with Tako-tsubo cardiomyopathy.J Cardiovasc Med (Hagerstown). 2009;10:100-3. Kuntjoro I, Teo SG, Poh KK.Electrocardiography series. Non-ischaemic causes of ST segment elevation.Singapore Med J. 2012;53:367-71. Looi JL, Wong CW, Lee M, et al. Usefulness of ECG to differentiate Takotsubo cardiomyopathy from acute coronary syndrome.Int J Cardiol. 2015;199:132-40. Masami K, Ebina T, Hibi K, et al. Differences in negative T waves among acute coronary syndrome, acute pulmonary embolism, and Takotsubo cardiomyopathy.Eur Heart J Acute Cardiovasc Care. 2012;1:349-57. Mugnai G, Pasqualin G, Benfari G, et al. Acute electrocardiographic differences between Takotsubo cardiomyopathy and anterior ST elevation myocardial infarction.J Electrocardiol. 2015;48:79-85. Parkkonen O, Allonen J, Vaara S, et al. Differences in ST-elevation and T-wave amplitudes do not reliably differentiate takotsubo cardiomyopathy from acute anterior myocardial infarction.J Electrocardiol. 2014;47:692-9. Zhong-qun Z, Chong-quan W, Sclarovsky S, et al. ST-segment deviation pattern of takotsubo cardiomyopathy similar to acute pericarditis: diffuse ST-segment elevation.J Electrocardiol. 2013;46:84-9. Santoro F, Brunetti ND, Tarantino N, et al. Dynamic changes of QTc interval and prognostic significance in takotsubo (stress) cardiomyopathy.Clin Cardiol. 2017;40:1116-22. Yamaguchi T, Yoshikawa T, Isogai T, et al. Predictive value of QRS duration at admission for in-hospital clinical outcome of Takotsubo cardiomyopathy.Circ J. 2016;81:62-8. Takashio S, Yamamuro M, Kojima S, et al. Usefulness of SUM of ST-segment elevation on electrocardiograms (limb leads) for predicting in-hospital complications in patients with stress (takotsubo) cardiomyopathy.Am J Cardiol. 2012;109:1651-6. Weihs V, Szücs D, Fellner B, et al. Electrocardiogram changes and wall motion abnormalities in the acute phase of Tako-Tsubo syndrome.Eur Heart J Acute Cardiovasc Care. 2016;5:481-8. Kasu S, Kato Y, Mitsuba N, et al. Comparison of electrocardiographic findings between the midventricular ballooning form and apical ballooning form of takotsubo cardiomyopathy.Clin Cardiol. 2011;34:555-9. Peters S.Takotsubo cardiomyopathy and electrocardiographic signs of perimyocarditis-findings of coronary angiography.Int J Cardiol. 2016;223:790. Núñez-Gil IJ, Luaces M, Garcia-Rubira JC, Zamorano J.Electrocardiographic criteria in Takotsubo cardiomyopathy and race differences: Asians versus Caucasians.J Am Coll Cardiol. 2010;56:1433-4.
REFERENCES
1. Duran-Cambra A, Sutil-Vega M, Fiol M, et al. Systematic review of the electrocardiographic changes in the Takotsubo syndrome. Ann Noninvasive Electrocardiol 2015; 20:1-6. https://doi.org/10.1111/anec.12228
PMid:25367822
2. Madias JE, Macfarlane PW. Artificial attenuation of ECG voltage produces shortening of the corresponding QRS duration: clinical implications for patients with edema. Pacing Clin Electrophysiol 2005; 28:1060-5. https://doi.org/10.1111/j.1540-8159.2005.00221.x
PMid:16221264
3. Frangieh AH, Obeid S, Ghadri JR, et al; InterTAK Collaborators. ECG criteria to differentiate between takotsubo (stress) cardiomyopathy and myocardial infarction. J Am Heart Assoc 2016; 5:e003418. https://doi.org/10.1161/JAHA.116.003418
PMid:27412903 PMCid:PMC4937281
5. Perazzolo Marra M, Zorzi A, Corbetti F, et al. Apicobasal gradient of left ventricular myocardial edema underlies transient T-wave inversion and QT interval prolongation (Wellens' ECG pattern) in Tako-Tsubo cardiomyopathy. Heart Rhythm 2013; 10:70-7. https://doi.org/10.1016/j.hrthm.2012.09.004
PMid:22975421
6. Mugnai G, Vassanelli F, Pasqualin G, et al. Dynamic changes of repolarization abnormalities in takotsubo cardiomyopathy. Acta Cardiol 2015; 70:225-32. https://doi.org/10.1080/AC.70.2.3073515
PMid:26148384
7. Hasdemir C, Vuran O, Yuksel A, Yavuzgil O. Stress cardiomyopathy (Tako-Tsubo) associated with sustained polymorphic ventricular tachycardia. Pacing Clin Electrophysiol 2013; 36:e111-4. https://doi.org/10.1111/j.1540-8159.2012.03431.x
PMid:22650252
8. Madias J. A patient with ventricular fibrillation and inverted Takotsubo syndrome triggered by sinus surgery: plausible causes, and electrocardiographic features. Turk Kardiyol Dern Ars 2016; 44:535. https://doi.org/10.5543/tkda.2016.22924
9. Namgung J. Electrocardiographic findings in Takotsubo cardiomyopathy: ECG evolution and its difference from the ECG of acute coronary syndrome. Clin Med Insights Cardiol 2014; 8:29-34. https://doi.org/10.4137/CMC.S14086
PMid:24653650 PMCid:PMC3956807
10. Valbusa A, Ingrassia S, Rosa GM, et al. Takotsubo cardiomyopathy and torsade de pointes in myasthenic crisis: be aware of QT prolongation. Am J Emerg Med 2013; 31:1717-8. https://doi.org/10.1016/j.ajem.2013.09.030
PMid:24161204
11. Cativo EH, Valvani R, Mene-Afejuku TO, Cativo DP, Mushiyev S. A rare association of Takotsubo cardiomyopathy with high-degree atrioventricular block. Case Rep Cardiol 2017; 2017:6989438.
12. Parodi G, Salvadori C, Del Pace S, et al; Tuscany Registry of Tako-Tsubo Cardiomyopathy. Left bundle branch block as an electrocardiographic pattern at presentation of patients with Tako-tsubo cardiomyopathy. J Cardiovasc Med (Hagerstown) 2009; 10:100-3. https://doi.org/10.2459/JCM.0b013e32831a6a26
13. Kuntjoro I, Teo SG, Poh KK. Electrocardiography series. Non-ischaemic causes of ST segment elevation. Singapore Med J 2012; 53:367-71.
PMid:22711033
14. Looi JL, Wong CW, Lee M, et al. Usefulness of ECG to differentiate Takotsubo cardiomyopathy from acute coronary syndrome. Int J Cardiol 2015; 199:132-40. https://doi.org/10.1016/j.ijcard.2015.07.046
PMid:26188834
15. Masami K, Ebina T, Hibi K, et al. Differences in negative T waves among acute coronary syndrome, acute pulmonary embolism, and Takotsubo cardiomyopathy. Eur Heart J Acute Cardiovasc Care 2012; 1:349-57. https://doi.org/10.1177/2048872612466790
PMid:24062927 PMCid:PMC3760560
16. Mugnai G, Pasqualin G, Benfari G, et al. Acute electrocardiographic differences between Takotsubo cardiomyopathy and anterior ST elevation myocardial infarction. J Electrocardiol 2015; 48:79-85. https://doi.org/10.1016/j.jelectrocard.2014.11.001
PMid:25465858
17. Parkkonen O, Allonen J, Vaara S, et al. Differences in ST-elevation and T-wave amplitudes do not reliably differentiate takotsubo cardiomyopathy from acute anterior myocardial infarction. J Electrocardiol 2014; 47:692-9. https://doi.org/10.1016/j.jelectrocard.2014.06.006
PMid:25022798
18. Zhong-qun Z, Chong-quan W, Sclarovsky S, et al. ST-segment deviation pattern of takotsubo cardiomyopathy similar to acute pericarditis: diffuse ST-segment elevation. J Electrocardiol 2013; 46:84-9. https://doi.org/10.1016/j.jelectrocard.2012.11.013
PMid:23276390
19. Santoro F, Brunetti ND, Tarantino N, et al. Dynamic changes of QTc interval and prognostic significance in takotsubo (stress) cardiomyopathy. Clin Cardiol 2017; 40:1116-22. https://doi.org/10.1002/clc.22798
PMid:28892227
20. Yamaguchi T, Yoshikawa T, Isogai T, et al. Predictive value of QRS duration at admission for in-hospital clinical outcome of Takotsubo cardiomyopathy. Circ J 2016; 81:62-8. https://doi.org/10.1253/circj.CJ-16-0912
PMid:27916778
21. Takashio S, Yamamuro M, Kojima S, et al. Usefulness of SUM of ST-segment elevation on electrocardiograms (limb leads) for predicting in-hospital complications in patients with stress (takotsubo) cardiomyopathy. Am J Cardiol 2012; 109:1651-6. https://doi.org/10.1016/j.amjcard.2012.01.393
PMid:22440122
22. Weihs V, Szücs D, Fellner B, et al. Electrocardiogram changes and wall motion abnormalities in the acute phase of Tako-Tsubo syndrome. Eur Heart J Acute Cardiovasc Care 2016; 5:481-8. https://doi.org/10.1177/2048872615598630
PMid:26228446
23. Kurisu S, Kato Y, Mitsuba N, et al. Comparison of electrocardiographic findings between the midventricular ballooning form and apical ballooning form of takotsubo cardiomyopathy. Clin Cardiol 2011; 34:555-9. https://doi.org/10.1002/clc.20934
PMid:21905042
24. Peters S. Takotsubo cardiomyopathy and electrocardiographic signs of perimyocarditis-findings of coronary angiography. Int J Cardiol 2016; 223:790. https://doi.org/10.1016/j.ijcard.2016.08.288
PMid:27573611
25. Nú-ez-Gil IJ, Luaces M, Garcia-Rubira JC, Zamorano J. Electrocardiographic criteria in Takotsubo cardiomyopathy and race differences: Asians versus Caucasians. J Am Coll Cardiol 2010; 56:1433-4. https://doi.org/10.1016/j.jacc.2010.06.025
PMid:20947004