Singapore Med J 2018; 59(4): 183-189 doi: https://doi.org/10.11622/smedj.2018046
Common accessory ossicles of the foot: imaging features, pitfalls and associated pathology
Bimal Mayur Kumar Vora1, MBBS, FRCR, Bak Siew Steven Wong2, MBChB, MMed
Author Information >Copyright and License information >
1Department of Diagnostic Radiology, Singapore General Hospital, Singapore 2Department of Radiology, Sengkang General Hospital, Singapore Correspondence: Dr Steven Bak Siew Wong, Senior Consultant, Department of Radiology, Sengkang General Hospital, c/o Alexandra Hospital, 378 Alexandra Road, Singapore 159964. steven.wong@singhealth.com.sg
Accessory ossicles are normal variants that are frequently seen but often overlooked or misdiagnosed. Commonly seen at the foot and ankle, they may be mistaken for fracture fragments or loose bodies, or not be recognised as a cause of the patient’s symptoms. This pictorial essay aimed to review commonly encountered accessory ossicles of the foot and ankle by highlighting anatomic landmarks and associated pathologic processes through the use of both basic and advanced imaging modalities, in an effort to increase awareness of these clinical entities.
Accessory ossicles are well-corticated bony structures found close to bones or a joint. They result from unfused ossification centres and are frequently congenital. They may, however, also be the result of prior trauma. Accessory ossicles can be found adjacent to various joints, such as the wrist, shoulder, hip or knee, but the foot and ankle are relatively common locations.
Accessory ossicles are usually an incidental finding on radiographs and often overlooked. At times, they mimic fractures or loose bodies, proving to be a diagnostic conundrum, thus leading to misdiagnoses. They may also contribute to or exacerbate underlying pathology, giving rise to symptoms. Higher modalities, such as computed tomography (CT), magnetic resonance (MR) imaging and even scintigraphy, are used in cases with diagnostic difficulty or when resulting pathology is suspected. This paper aimed to provide a pictorial representation of the more commonly encountered accessory ossicles of the foot and ankle, and showcase their anatomic features, resulting pathology and potential pitfalls in diagnosis.
ACCESSORY NAVICULAR
Three types of accessory navicular have been described. Type 1 accessory navicular (Fig. 1) is found within the posterior tibial tendon, close to its attachment to the navicular, and makes up about 30% of cases. It is typically small, measuring about 2–3 mm in size, does not have a cartilaginous interface with the navicular and is considered to be a sesamoid bone of the posterior tibial tendon.(1) Type 2 accessory navicular (Fig. 2), seen in about 50% of cases, is located close to the median eminence of the navicular bone, forming a flat facet with an intervening synchondrosis, which is a cartilaginous interface between the accessory navicular and the navicular bone. Type 3 accessory navicular (Fig. 3), which makes up the remaining 20% of cases, is a fused ossification centre, resulting in a prominent median eminence,(1) and there is no synchondrosis. The accessory navicular is bilateral in about 50% of cases(2) and is more common in women. Its overall prevalence is about 2%–21%, making it the second most common accessory ossicle.(2)
Fig. 1
Type 1 accessory navicular. Axial CT image of the foot shows an ossicle (arrow) measuring about 3 mm in size, adjacent to the navicular (asterisk) and within the tibialis posterior tendon.
Fig. 2
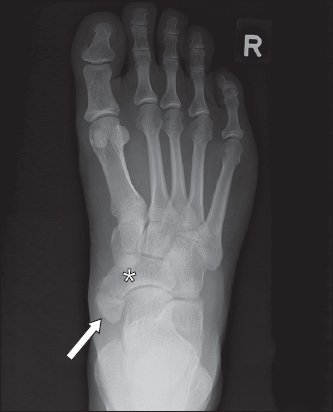
Type 2 accessory navicular. Right foot radiograph shows an accessory navicular (arrow) forming a flat facet with an intervening synchondrosis at the median eminence of the navicular (asterisk).
Fig. 3
Type 3 accessory navicular. Left foot radiograph shows an accessory navicular that has fused with the navicular bone (asterisk), resulting in a prominent median eminence (arrow).
Of the three types of accessory navicular, Type 2 is most commonly symptomatic, presenting as medial foot pain.(3) This is also known as os naviculare syndrome. Shear stress at the synchondrosis caused by pull of the posterior tibial tendon is thought to be a cause.(4) MR imaging is usually required to establish the diagnosis in symptomatic cases. Bone marrow oedema of the accessory navicular and the articulating navicular (Fig. 4), and thickening of the posterior tibial tendon (Fig. 5) are some features that may be observed in os naviculare syndrome.(5) Posterior tibial tendon tears may also be seen.(5)
Fig. 4
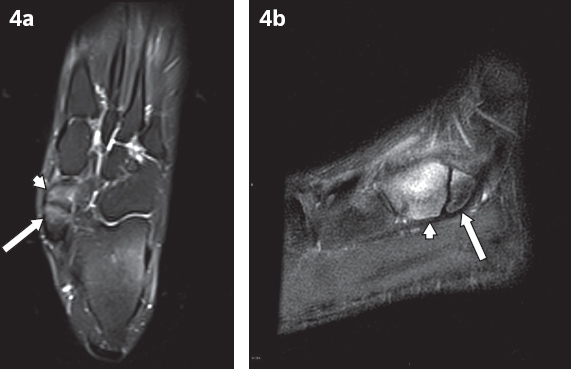
Os naviculare syndrome. (a) Axial and (b) sagittal T2-W MR images from two different patients with medial foot pain and tenderness show bony oedema in Type 2 accessory naviculars (arrows in a & b) and the navicular bones (arrowheads in a & b) across the synchondrosis, as shown by increased T2-W signal within the bones.
Fig. 5
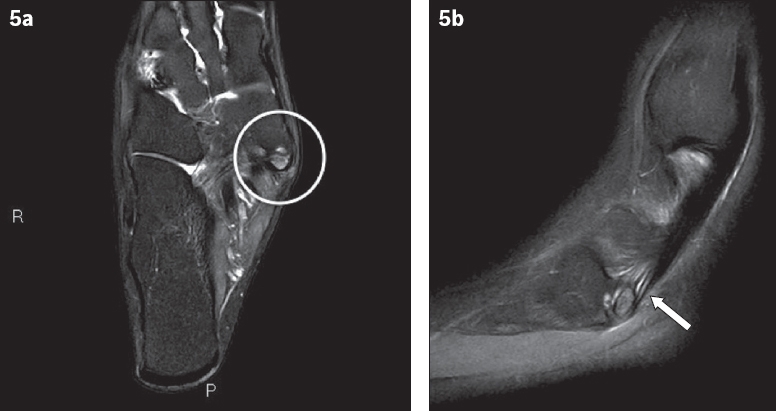
Painful accessory navicular. (a) Axial T2-W MR image shows bony oedema in both the accessory ossicle and adjacent navicular bone (circle). (b) Sagittal MR image shows oedema (arrow) in the tibialis posterior tendon, in keeping with accessory navicular syndrome.
OS TRIGONUM
The os trigonum is situated posteriorly to the talus and may be triangular or ovoid in shape (Fig. 6). A synchondrosis exists between the ossicle and the talus. The os trigonum has a reported prevalence of 7%–25%(2) and is best seen on the lateral projection.
Fig. 6
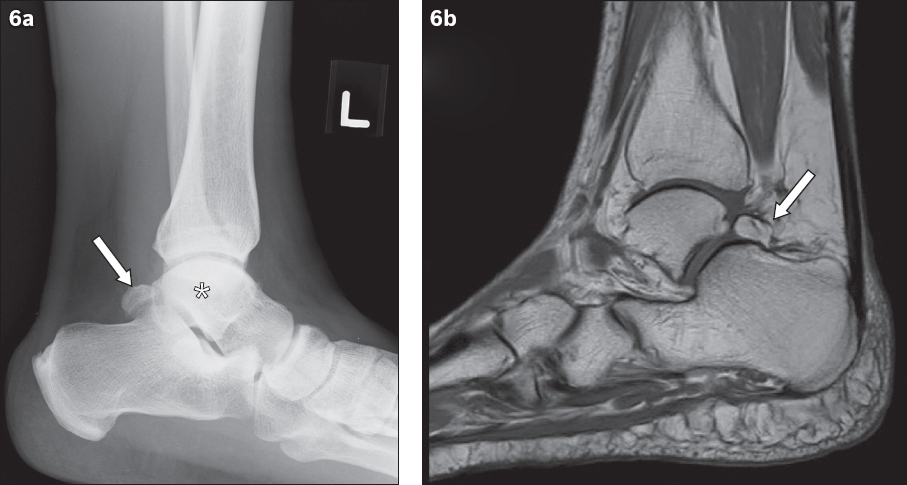
Os trigonum. (a) Lateral radiograph of the ankle shows an ovoid bony structure (arrow) posterior to the talus (asterisk). The structure is well corticated, likely representing an os trigonum rather than a fracture. (b) Sagittal T1-weighted MR image shows an os trigonum (arrow) with a synchondrosis between the ossicle and talus.
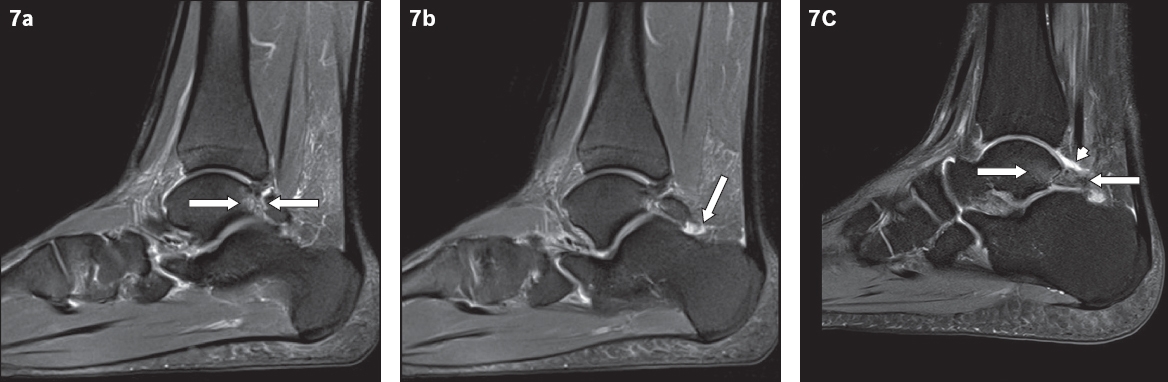
The os trigonum may contribute to posterior ankle impingement syndrome (Figs. 7 & 8), which is associated with repeated plantar flexion,(6) and presents as posterior ankle pain and swelling. Imaging findings include soft tissue swelling, synovitis and flexor hallucis longus (FHL) tendon tenosynovitis. The FHL tendon traverses medially to the os trigonum, and repetitive stress or compression to the tendon with plantar flexion can result in inflammation (Fig. 8).(7) Chronic impingement can result in degenerative change at the synchondrosis, with cystic and sclerotic changes on both sides of the synchondrosis.
Fig. 7
Posterior ankle impingement syndrome. (a & b) Sagittal T2-W MR images show bony oedema (arrows in a) in the ossicle and posterior talus at the synchondrosis. There is also synovitis with a small effusion (arrow in b) at the posterior ankle. (c) Sagittal MR image of the ankle of a 26-year-old man who presented with posterior ankle pain also shows bony oedema (arrows) in the posterior talus and os trigonum, with a small joint effusion (arrowhead).
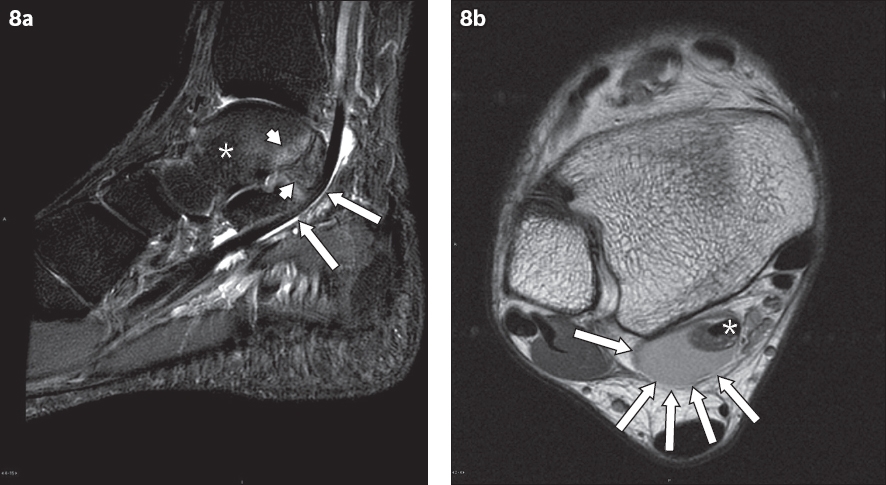
Fig. 8
Posterior ankle impingement syndrome. (a) Sagittal T2-W MR image shows bony oedema (arrowheads) in the talus (asterisk) and os trigonum posteriorly, with fluid surrounding the flexor hallucis longus tendon (arrows), which suggests tenosynovitis. (b) Axial proton-density MR image of the same patient with posterior impingement better demonstrates the fluid (arrows) surrounding the flexor hallucis longus tendon (asterisk), which suggests tenosynovitis.
A differential diagnosis for a bony opacity that is posterior to the talus is a fracture of the fused trigonal process of the talus, which may result from forceful plantar flexion. It also results in posterior ankle pain, but in this case, knowing the acute history of the pain would be helpful in diagnosis.(6) Another common differential is a fracture of the lateral process of the talus (i.e. Shepherd’s fracture).(2,6)
OS PERONEUM
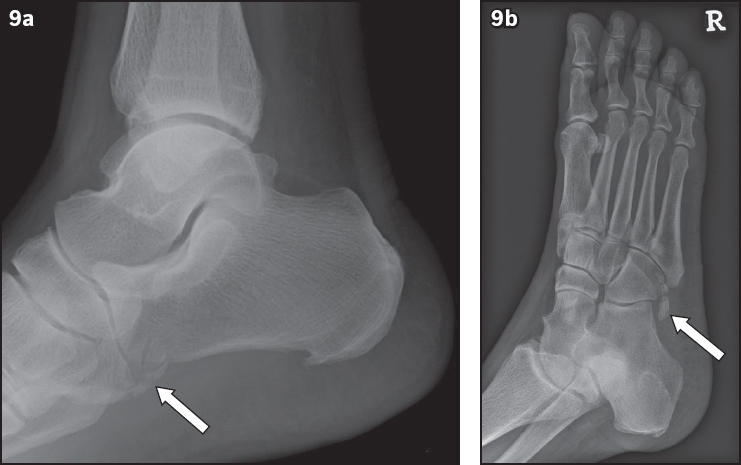
The os peroneum is located adjacent to the calcaneocuboid joint (Fig. 9) and embedded within the peroneus longus tendon. It is best seen on lateral or oblique views of the foot. The os peroneum may be bipartite in 30% of cases and bilateral in 60% of cases.(8)
Fig. 9
Os peroneum. (a) Lateral ankle radiograph shows a few bony opacities (arrow) projected over the calcaneocuboid joint in an 81-year-old patient who presented with ankle pain. This represents the os peroneum which, in this case, appears fragmented. (b) This is similarly witnessed on the oblique view (arrow), raising the possibility of a fracture of the ossicle. MR imaging was subsequently performed.
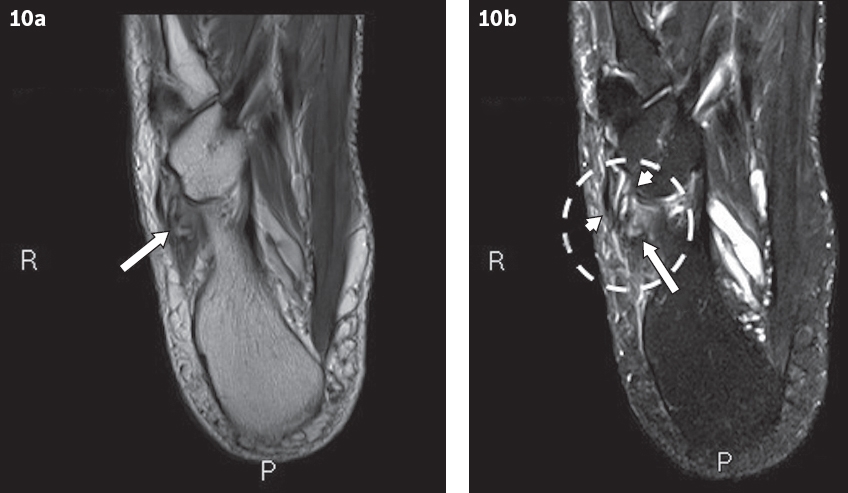
The os peroneum may become symptomatic, presenting as lateral foot pain(9) and tenderness, which is also known as painful os peroneum syndrome. This can be due to fracture of the ossicle (Fig. 10) or degeneration.(8) It can result in a tear of the peroneus longus tendon that is evidenced by a displaced os peroneum on imaging.(10) MR imaging (Fig. 10) may show abnormal T2 signal within the ossicle and tendinosis of the peroneus longus tendon.(2) Ultrasonography may also be used to demonstrate inflammatory change in the soft tissue, and tendon tears or tenosynovitis of the peroneus longus tendon.(10)
Fig. 10
(a) Axial T1-W MR image of the patient from Fig. 9 shows a fragmented os peroneum (arrow) in the thickened peroneus longus tendon. (b) T2-W MR image shows bony oedema in the os peroneum (arrow). The peroneus longus tendon is oedematous in the region of the ossicle (circle), with suggestion of a split tear (arrowheads). This is suggestive of a fracture of the os peroneum and probably explains the patient’s pain.
OS VESALIANUM
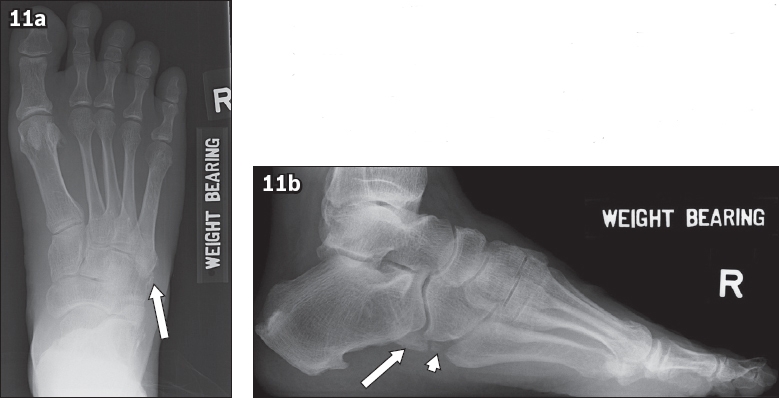
The os vesalianum (Fig. 11) is situated proximal to the base of the fifth metatarsal, within the peroneus brevis tendon.(2) It may be seen in about 0.1%–1.0% of individuals(11) and must be differentiated from an apophysis of the fifth metatarsal, which is oriented parallel to the metatarsal shaft. The os vesalianum rarely causes symptoms. In the setting of pain, other diagnoses should also be considered, such as a fracture of the fifth metatarsal base or apophysitis, which is inflammation of the apophysis at the fifth metatarsal base.
Fig. 11
Os vesalianum. (a) Right foot radiograph shows an os vesalinum (arrow) proximal to the fifth metatarsal base. The differential for a bony opacity in this region is an unfused apophysis orientated parallel to the cortex of the metatarsal base. (b) Lateral projection of the right foot radiograph of the same patient shows two accessory ossicles, an os peroneum proximally (arrow) and a smaller os vesalianum (arrowhead) distally.
OS INTERMETATARSEUM
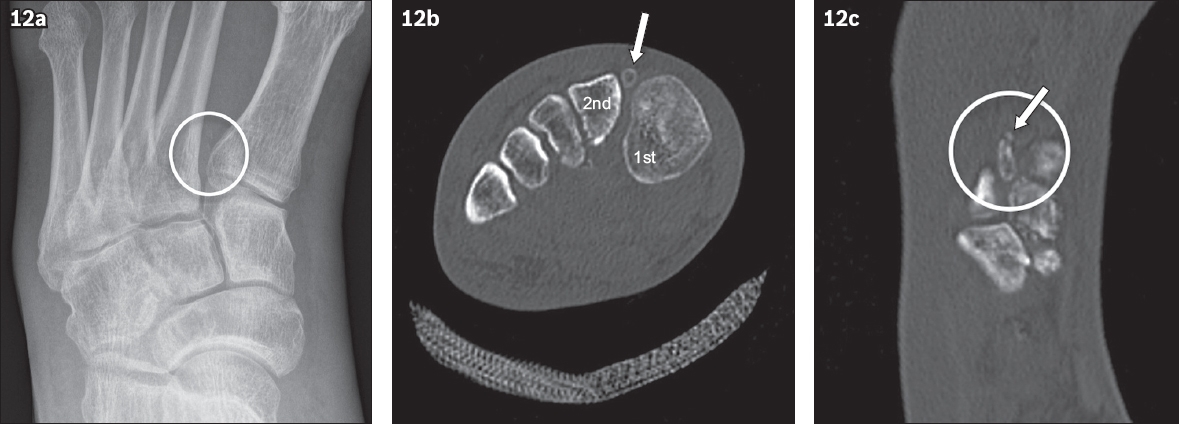
The os intermetatarseum (Fig. 12) is situated between the first and second metatarsals. Three types have been described; it may be (a) free-standing, having no articulation with the adjacent bones; (b) articulating, forming a joint between the first or second metatarsal bases and/or the medial cuneiform, in any combination; (c) fused, arising as a spur from any of the adjacent bones. The reported incidence shows variation between anatomical studies (up to 13%) and radiological studies (up to 7%).(2) This variation may be due to the difficulty in identifying these small ossicles that can be easily obscured on radiographs by adjacent bony structures.
Fig. 12
Os intermetatarseum. (a) Foot radiograph and (b) coronal CT image show a bony opacity (circle in a & arrow in b) between the bases of the first and second metatarsals. (c) CT image shows that the bony opacity is well corticated, apart from a fracture at its distal aspect (arrow). This is in keeping with a fractured os intermetatarseum.
This ossicle may occasionally be symptomatic, presenting as dorsal foot pain or paraesthesia with numbness over the first intermetatarsal space, probably due to compression of the branches of the deep peroneal nerve.(12,13) The onset usually follows trauma, with other reported inciting factors such as tight footwear and cavus feet.(12) The os intermetatarseum may also be mistaken for a fracture at the base of the second metatarsal, which occurs in Lisfranc injuries. We present a case of a fractured os intermetatarseum in a patient post-trauma (Fig. 12).
Symptomatic os intermetatarseum is usually treated conservatively with nonsteroidal anti-inflammatory drugs and footwear or activity modification, failing which, surgical excision may be considered.(12)
SESAMOIDS
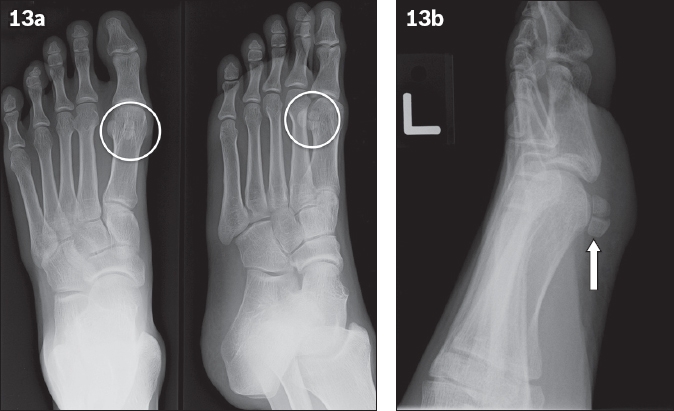
Sesamoids of the foot can be subdivided into hallucal, interphalangeal joint and lesser metatarsal sesamoids.(2) In humans, hallucal sesamoids are invariably present. Hallucal sesamoids have medial and lateral components (Fig. 13). They can be bipartite, which is usually seen in the medial sesamoid if this occurs.
Fig. 13
(a & b) Radiographs show that the medial sesamoid of the first metatarsal is made out of two parts (circles in a & arrow in b). Both parts are well corticated. Hence, this is probably a bipartite sesamoid rather than an acute fracture. Old fractures that have healed can, however, have a similar appearance.
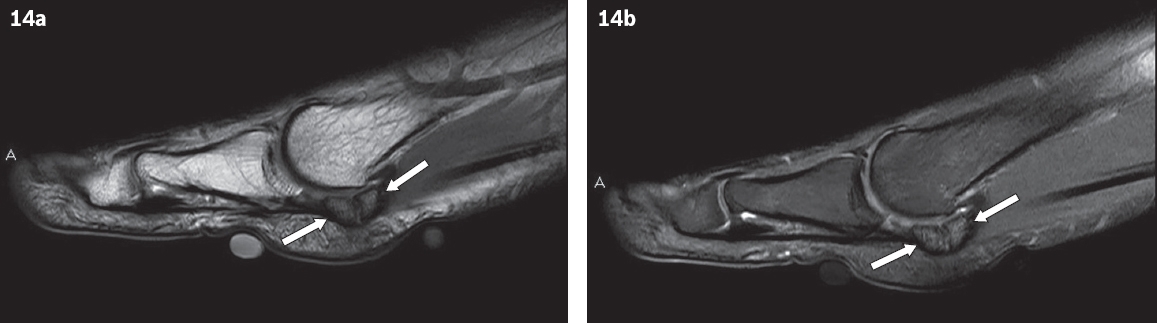
A common pitfall is mistaking a bipartite sesamoid for a fractured sesamoid. Other pathologies involving sesamoids include degenerative change, infection and osteonecrosis.(2) Chronic pain over the sesamoids, often referred to as sesamoiditis, can occur from chronic stress and repetitive injury to the sesamoid. It most commonly involves the hallucal sesamoid. MR imaging (Fig. 14) is useful for diagnosis and shows abnormal signals in the sesamoids and surrounding soft tissue inflammation (i.e. tendinitis or synovitis).(2,14,15) Bone scintigraphy may also be helpful in difficult cases to show increased tracer uptake in the sesamoids.(2,15)
Fig. 14
A patient experienced chronic pain over the metatarsal head and was suspected to have sesamoiditis. (a) Sagittal T1-W MR image shows low T1-W signal in the medial sesamoid (arrows). (b) Sagittal T2-W MR image shows increased signal in the medial sesamoid (arrows) indicating bony oedema, which is suspicious for sesamoiditis.
CONCLUSION
There are many different accessory ossicles of the foot, only some of which have been featured in this article. It is important to recognise the existence of these ossicles, as they can be an important cause of a patient’s symptoms. Being cognisant of these ossicles also prevents us from misdiagnosing them as fractures in the setting of foot pain, which is a commonly encountered situation. Apart from radiographs, advanced imaging techniques such as CT, MR imaging and even ultrasonography or nuclear medicine techniques can be helpful in establishing the diagnosis in difficult cases and evaluating foot pain secondary to accessory ossicles.
References Lawson JP, Ogden JA, Sella E, Barwick KW.The painful accessory navicular.Skeletal Radiol. 1984;12:250-62. Nwawka OK, Hayashi D, Diaz LE, et al. Sesamoids and accessory ossicles of the foot:anatomical variability and related pathology.Insights Imaging. 2013;4:581-93. Miller TT.Painful accessory bones of the foot.Semin Musculoskelet Radiol. 2002;6:153-61. Sella EJ, Lawson JP, Ogden JA.The accessory navicular synchondrosis.Clin Orthop Relat Res. 1986;209:280-5. Choi YS, Lee KT, Kang HS, Kim EK.MR imaging findings of painful type II accessory navicular bone:correlation with surgical and pathologic studies.Korean J Radiol. 2004;5:274-9. Lee JC, Calder JD, Healy JC.Posterior impingement syndromes of the ankle.Semin Musculoskelet Radiol. 2008;12:154-69. Lo LD, Schweitzer ME, Fan JK, Wapner KL, Hecht PJ.MR imaging findings of entrapment of the flexor hallucis longus tendon.AJR Am J Roentgenol. 2001;176:1145-8. Sobel M, Pavlov H, Geppert MJ, et al. Painful os peroneum syndrome:a spectrum of conditions responsible for plantar lateral foot pain.Foot Ankle Int. 1994;15:112-24. GökkuÅ K, Sagtas E, Demirci E, Saylik M, Aydın AT.Degenerative arthritis of pseudoarticulation between the os peroneum and cuboid:a rare cause of lateral foot pain.Foot Ankle Surg. 2015;21:e9-e11. Brigido MK, Fessell DP, Jacobson JA, et al. Radiography and US of os peroneum fractures and associated peroneal tendon injaes:initial experience.Radiology. 2005;237:235-41. Boya H, Ozcan O, TandoÄan R, Günal I, Araç S.Os vesalianum pedis.J Am Podiatr Med Assoc. 2005;95:583-5. Nakasa T, Fukuhara K, Adachi N, Ochi M.Painful os intermetatarseum in athletes:report of four cases and review of the literature.Arch Orthop Trauma Surg. 2007;127:261-4. Summers A.Accessory ossicles and sesamoid bones:recognition and treatment.Emerg Nurse. 2015;22:27-32. Ashman CJ, Klecker RJ, Yu JS.Forefoot pain involving the metatarsal region:differential diagnosis with MR imaging.Radiographics. 2001;21:1425-40. Mellado JM, Ramos A, Salvadó E, et al. Accessory ossicles and sesamoid bones of the ankle and foot:imaging findings, clinical significance and differential diagnosis.Eur Radiol. 2003;13:Suppl 6L164-77.
REFERENCES:
1. Lawson JP, Ogden JA, Sella E, Barwick KW. The painful accessory navicular. Skeletal Radiol 1984; 12:250-62. https://doi.org/10.1007/BF00349506
PMid:6239377
2. Nwawka OK, Hayashi D, Diaz LE, et al. Sesamoids and accessory ossicles of the foot: anatomical variability and related pathology. Insights Imaging 2013; 4:581-93. https://doi.org/10.1007/s13244-013-0277-1
PMid:24006205 PMCid:PMC3781258
3. Miller TT. Painful accessory bones of the foot. Semin Musculoskelet Radiol 2002; 6:153-61. https://doi.org/10.1055/s-2002-32361
PMid:12077704
5. Choi YS, Lee KT, Kang HS, Kim EK. MR imaging findings of painful type II accessory navicular bone: correlation with surgical and pathologic studies. Korean J Radiol 2004; 5:274-9. https://doi.org/10.3348/kjr.2004.5.4.274
PMid:15637478 PMCid:PMC2698172
6. Lee JC, Calder JD, Healy JC. Posterior impingement syndromes of the ankle. Semin Musculoskelet Radiol 2008; 12:154-69. https://doi.org/10.1055/s-2008-1078703
PMid:18509795
7. Lo LD, Schweitzer ME, Fan JK, Wapner KL, Hecht PJ. MR imaging findings of entrapment of the flexor hallucis longus tendon. AJR Am J Roentgenol 2001; 176:1145-8. https://doi.org/10.2214/ajr.176.5.1761145
PMid:11312169
8. Sobel M, Pavlov H, Geppert MJ, et al. Painful os peroneum syndrome: a spectrum of conditions responsible for plantar lateral foot pain. Foot Ankle Int 1994; 15:112-24. https://doi.org/10.1177/107110079401500306
PMid:7951939
9. Gökkuş K, Sagtas E, Demirci E, Saylik M, Aydın AT. Degenerative arthritis of pseudoarticulation between the os peroneum and cuboid: a rare cause of lateral foot pain. Foot Ankle Surg 2015; 21:e9-e11. https://doi.org/10.1016/j.fas.2014.08.011
PMid:25682421
10. Brigido MK, Fessell DP, Jacobson JA, et al. Radiography and US of os peroneum fractures and associated peroneal tendon injuries: initial experience. Radiology 2005; 237:235-41. https://doi.org/10.1148/radiol.2371041067
PMid:16183934
11. Boya H, Ozcan O, Tandoğan R, Günal I, Araç S. Os vesalianum pedis. J Am Podiatr Med Assoc 2005; 95:583-5. https://doi.org/10.7547/0950583
PMid:16291851
12. Nakasa T, Fukuhara K, Adachi N, Ochi M. Painful os intermetatarseum in athletes: report of four cases and review of the literature. Arch Orthop Trauma Surg 2007; 127:261-4. https://doi.org/10.1007/s00402-006-0195-5
PMid:16850328
13. Summers A. Accessory ossicles and sesamoid bones: recognition and treatment. Emerg Nurse 2015; 22:27-32. https://doi.org/10.7748/en.22.10.27.e1404
PMid:25746889
15. Mellado JM, Ramos A, Salvadó E, et al. Accessory ossicles and sesamoid bones of the ankle and foot: imaging findings, clinical significance and differential diagnosis. Eur Radiol 2003; 13 Suppl 6:L164-77. https://doi.org/10.1007/s00330-003-2011-8