

Abstract
Early cardiopulmonary resuscitation (CPR) and defibrillation prior to the arrival of emergency medical services can improve survival from out-of-hospital cardiac arrest (OHCA) with good neurological outcome. However, the rate of local bystander CPR is only 24.3% and bystander defibrillation 2.1%. In 2015, the R-AEDI (Registry for AED Integration) initiative was started to improve OHCA survival rates. R-AEDI alerts volunteers to nearby OHCA cases via the myResponder mobile application. In 2015–2017, 7,682 AEDs were mapped and made accessible via this app. Comprehensive site inspections also resulted in fewer non-functional AEDs, as AED owners were educated on the importance of the maintenance of pads and batteries. The AED heat map allows us to identify areas that are lacking in or require improved public access AED coverage. The online AED registry found in the myResponder app is useful to locate AEDs rapidly during OHCAs. More community education would improve the rate of bystander defibrillation.
INTRODUCTION
Out-of-hospital cardiac arrest (OHCA) is a global health issue that affects around 350,000 Americans(1) and 275,000 Europeans(2) annually. Effective treatment of OHCA hinges on Cummins’ ‘chain of survival’ – immediate recognition of cardiac arrest and activation of the emergency response system, early cardiopulmonary resuscitation (CPR), early defibrillation, and early advanced life support.(3) The medical literature has tended to focus more on hospital and advanced life support treatment rather than community treatment and basic life support.(4) However, there is increasing recognition that early CPR and defibrillation prior to the arrival of emergency medical services (EMS) can help to improve OHCA survival with good neurological outcome.(5,6)
The latest American Heart Association statistics revealed that bystander CPR occurred in 43.6% of OHCA cases in the United States, but automated external defibrillator (AED) usage occurred in only 6.7% of cases.(1) There was a similar trend in Singapore: bystander CPR occurred in 24.3% of OHCA cases, while the rate of bystander defibrillation was 2.1%.(7) A recent systematic review identified key barriers to the use of public access defibrillators (PADs), including problems locating AEDs, poor accessibility, limited availability and lack of information sharing.(8) This paper highlights initiatives that use smart technology to improve the survival rates of OHCA victims in Singapore.
MYRESPONDER APP AND AED REGISTRY
MyResponder is a local first responder geolocation application that was launched on 17 April 2015. It uses crowdsourcing to increase bystander CPR rates by alerting volunteer first responders who are within 400 m of an OHCA victim. Anyone in Singapore can become a first responder after registration, simply by entering their local mobile number and NRIC/FIN (National Registration Identity Card/Foreign Identification Number). The app also shows the location of the nearest AED on the map, allowing others to assist by retrieving the AED. As seen on the app, as of 28 January 2019, there were 39,127 registered responders and 18,871 responses to cases.
At the same time, the Registry for AED Integration (R-AEDI) initiative was developed to improve the management of public AEDs and assist dispatchers and the public to increase AED usage. This collaboration between the Singapore Civil Defence Force (SCDF) and Singapore Heart Foundation (SHF) comprises two key components: (a) alerting volunteers to nearby OHCA cases via the myResponder app; and (b) building a national registry of PADs. Since 10 July 2015, the SHF has been engaged by the Ministry of Home Affairs (MHA) to promote the R-AEDI project. The SHF is responsible for the establishment and maintenance of the national AED registry, with a target of 6,000 AEDs in the registry by the end of 2018.
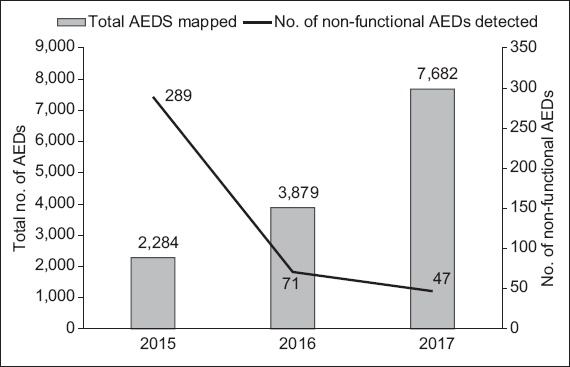
With the engagement of the SHF, the locations of all existing AEDs in the registry are verified, audited and updated. The AED’s serial number is also recorded, alongside the brand, model and expiry dates of pads and batteries. From 2015 to 2017, 7,682 AEDs were mapped in Singapore (
Fig. 1
Chart shows the number of AEDs in the registry and the number of non-functional AEDs detected each year. AED: automated external defibrillator
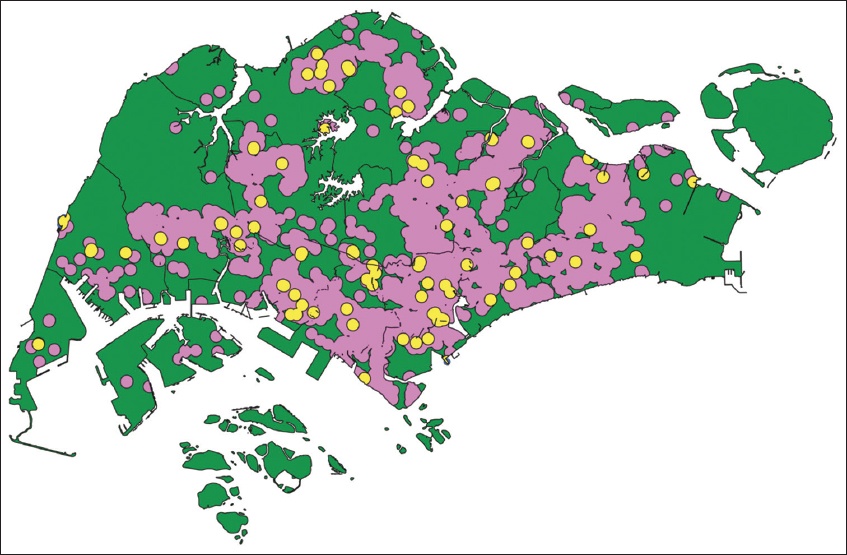
The local AED map is shown in
Fig. 2
Map shows the distribution of AEDs in Singapore. Areas that have public access AEDs within 400 m are highlighted in purple, while the yellow circles represent AEDs meant for private use. AED: automated external defibrillator
NEED FOR AN AED REGISTRY
Despite the life-saving potential of AEDs, their effectiveness is time-dependent, as ventricular fibrillation will become refractory to defibrillation, eventually degenerating into asystole. The probability of survival rapidly declines by 7%–10% with every minute of delay in defibrillation.(10) To date, AEDs are not capable of broadcasting location or status data electronically. Thus, an accurate, easily accessible AED map can help people to locate them in an emergency, either directly through smartphone applications or through communication with EMS.(11)
Over the years, some private and public organisations installed AEDs in various locations, but as there was no national AED registry prior to 2013, the public and the SCDF 995 control room were unaware of the existence of these AEDs.(12) Due to the absence of servicing contracts, maintenance of the AEDs was performed by the individual organisations, who, due to the low utility, may not be aware of the need for regular battery and pad replacement. In 2014, the MHA started the first AED leasing contract for public access AEDs under the Save-A-Life scheme, which bundled the cost of maintenance with that of replacement batteries and pads. Their upfront cost is much lower compared to individual AED purchases, making AEDs more affordable for building and business owners. Any damage or theft will be handled by the leasing company and regular CPR and AED training can also be provided for designated providers as part of this programme, to maintain currency.
CONTINUOUS EDUCATION
The local bystander defibrillation rate of 2.1%(7) pales in comparison to 3.5% in Taiwan(13) and 3.8% in Copenhagen, Denmark.(14) According to a local population-based survey conducted in 2009, 31.4% of participants were CPR-trained and 10.7% were AED-trained.(15) In addition, only 57.2% believed that they should be trained in AED as compared to 82.6% for CPR.
To promote the importance of CPR and AED and usage of myResponder during cardiac arrest, the SHF conducted roadshows and used online resources to publish survivors’ stories. Various CPR and AED training programmes are available. The DARE (Dispatcher-Assisted first REsponder) programme is a simplified 45-minute session in which participants watch a scenario-based video, then have a hands-on session to learn to dial 995 in an emergency, perform CPR as directed by the dispatcher, and use an AED. The full CPR and AED certification course is available for those who wish to learn more.
Due to limitations in Singapore’s existing legislation, several issues are not addressed by R-AEDI. Firstly, the AED registry is not legally mandated. There is no legal requirement for AED owners to share information about AED locations. AED owners have also expressed concerns related to cost and liability if the public use their AEDs. There is also no requirement for building owners to have AEDs, or to provide CPR and AED training.
The absence of a Good Samaritan law may also deter bystanders from using AEDs. Without AED laws, there are no requirements for high-risk locations to install AEDs. Most AEDs today also record data when activated, and this valuable information helps in understanding the interactions between the OHCA victim and the rescuers. In some states in the United States, evaluation of each OHCA event was required so as to develop a quality improvement plan.(16) There is great value in being able to retrieve and study this data.
Last but not least, the myResponder app is unable to discern whether the community first responders, who are self-registered, are genuinely trained in CPR and AED. However, the responders are reminded to attend the DARE programme for training and to render assistance only if they are trained.
THE WAY AHEAD
As mentioned earlier, there are some key barriers to the use of PADs. R-AEDI helps in locating AEDs via myResponder, which has now incorporated AED availability on the map – whether it is available 24/7 or limited to the operating hours of the compound. Future developments may include gamification so that the public can contribute location-based updates for public AEDs. The SHF has also created an AED pads replacement and subsidy programme to encourage AED owners to allow public usage of their AEDs.
Since the mid-1990s, legislatures across the United States began enacting AED-related laws, including Good Samaritan laws, hoping that these would reduce liability and encourage more organisations and individuals to buy or lease AEDs for public access. Such laws now exist in every state and vary in structure, content, complexity and scope of coverage. Locally, it has been encouraging that despite the absence of an AED law and Good Samaritan laws, Singaporeans have been coming forward to assist in the resuscitation of OHCA cases.
CONCLUSION
To improve the survival rates of OHCA victims in Singapore, it is imperative that we concentrate on community efforts to encourage primary prevention through leading a healthy lifestyle, early recognition of OHCA patients and prompt institution of life-saving measures. The Singapore Resuscitation and First Aid Council has set a target of having at least one first responder who is able to initiate early and prompt life-saving first aid in every household in Singapore by 2020. Through the community efforts initiated by the R-AEDI and Save-A-Life projects, it is hoped that bystander CPR and AED use will continue to increase in Singapore.
ACKNOWLEDGEMENTS
The authors would like to thank CPT Carl Ross de Souza from the Singapore Civil Defence Force as well as Mr Kenneth See, Mr Lim Kiat and the team from the SHF for their contribution towards the publication of this paper.