

Dear Sir,
The Ministry of Health, Singapore, published the National Infection Prevention and Control Guidelines for Acute Healthcare Facilities on 24 October 2017. The guidelines recommend conducting catheter-associated urinary tract infection (CAUTI) risk assessments to identify areas for improvement.(1) However, published data on CAUTI rates in Singapore remains surprisingly scarce, being limited to two reports from intensive care units (ICUs).(2,3) Herein, we report the first hospital-wide study on CAUTI rates in Singapore, which included data from the general wards.
As part of our hospital’s infection prevention surveillance programme, we reviewed patients admitted to Ng Teng Fong General Hospital, Singapore, from 1 February 2016 to 30 April 2016. Patients with urinary catheters during their hospitalisation were identified through the electronic medical record (EMR) system (Epic Systems Corporation, Verona, WI, USA). Their records were reviewed for CAUTI, as defined by United States National Healthcare Safety Network (NHSN) 2016 surveillance definitions.
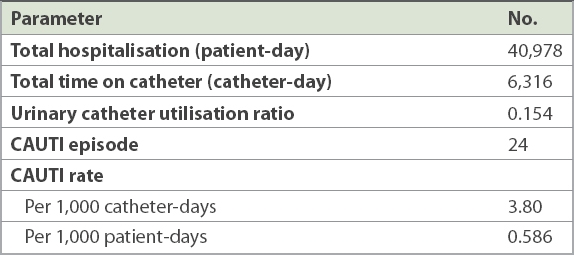
Patient admissions totalled 40,978 patient-days within the review period. There were 6,316 catheter-days and 24 CAUTI episodes. The catheter utilisation ratio of 0.154 was calculated by dividing the number of catheter days by the number of patient-days. CAUTI rates were calculated to be 3.80 per 1,000 catheter-days and 0.586 per 1,000 patient-days. Results are summarised in
Table I
Catheter utilisation ratio and catheter-associated urinary tract infection (CAUTI) rates observed over three months.
The burden of healthcare-associated infections (HAIs) on patient morbidity and mortality is well recognised. CAUTIs are the commonest HAI, with an estimated attributable cost of USD 862–1,007 per patient (2007 value, adjusted for consumer price index).(5) Based on a systematic review and meta-analysis of seven studies from Southeast Asia, mostly conducted in ICUs, the regional burden of CAUTIs was estimated to be 8.9 per 1,000 catheter-days.(6) Another recent ICU study from Singapore reported much lower CAUTI rates of 0.012 per 1,000 catheter-days.(2) However, to our knowledge, there has been no local data published regarding hospital-wide CAUTI rates, despite the burden of urinary catheter utilisation being highest among general ward patients.
Our study provides the first published hospital-wide CAUTI rates in a Singapore general hospital and suggests that CAUTI rates can be improved. The World Health Organization’s guidelines on infection prevention and control strongly recommend HAI surveillance, which is associated with reductions in the number of HAIs.(7) However, HAI surveillance is often a manpower-intensive endeavour. This study demonstrates that hospital EMR systems can be leveraged to establish a hospital-wide CAUTI surveillance system with minimal resources, thereby allowing us to identify targets and measure rates efficiently for use in infection prevention interventions.
Yours sincerely,