

Abstract
INTRODUCTION:
The increasing popularity of personal mobility devices (PMDs) and electric bicycles (e-bikes) in Singapore has met with growing public concern over safety. Following the passing of the Active Mobility Bill, there remains a gap in the local literature in terms of injury patterns arising from the use of these devices.
METHODS:
A retrospective study was conducted on the Singapore National Trauma Registry (SNTR) from the emergency department of an acute hospital from 1 January 2016 to 31 December 2016. All patients with injuries related to the use of PMDs and e-bikes were included. Data captured included demographic information, device used and injury severity score (ISS).
RESULTS:
The 259 patients identified had a mean age of 32.1 years and a male predominance. Most (83.4%) were injured from falling off their devices. Devices commonly associated with injury were scooters, skateboards and motorised bicycles. Most injuries were mild (94.6%, ISS < 9) and were mainly external wounds (89.2%) and upper and lower limb injuries (35.5%). There was no difference in ISS in terms of the device used (motorised vs. non-motorised). More severe injuries (ISS ≥ 9) were caused by e-bikes (42.9%) and electric scooters (28.6%). Factors associated with these injuries were older age, use of e-bikes, and injuries to the head, face and thorax. Most patients (86.1%) were discharged and one died.
CONCLUSION:
While most injuries associated with PMDs and e-bikes are minor, serious injuries could result from their use. The SNTR should be updated to include PMDs and e-bikes as a category.
INTRODUCTION
Personal mobility devices (PMDs) and electric bicycles (e-bikes) have become increasingly popular in Singapore in recent years, given their convenience and efficiency for short-distance travel and greater affordability. Utilised for leisure and commuting, they are widely regarded as an essential part of the country’s efforts towards a greener and ‘car-lite’ society.(1) This development is consistent with trends across the globe,(2) both in terms of sales and acceptance.(3,4) At the same time, there is growing concern for public safety following a series of high-profile accidents, especially those involving electric-powered forms of PMDs.(5) Video footage of a food delivery e-scooterist being hit by a car on a zebra crossing went viral in 2017.(6) The number of accidents involving e-bikes reported to the Traffic Police in Singapore has also increased from 39 in 2015 to 54 in 2016.(7)
Recommendations proposed by the Active Mobility Advisory Panel on the rules and code of conduct for cycling and use of PMDs were accepted by the Singapore government in 2016. These measures aim to meet challenges in public safety arising from the use of PMDs and power-assisted bicycles.(8) An Active Mobility Campaign was also launched in the same year to increase the public’s awareness of the proper use of these devices, with concurrent enforcement deployments across the country.(9) In January 2017, the recommendations were legislated with the passing of the Active Mobility Bill in Parliament.(10)
The literature is replete with studies on injuries from non-motorised PMDs such as kick-off scooters, roller blades and skateboards, and data on motorised PMDs is also gradually emerging overseas.(3,11) Nevertheless, there is a lack of published data on injury patterns arising from the use of PMDs in Singapore, especially those that are electrical and motorised. This information could inform healthcare providers about the type and spectrum of injuries that should be anticipated and guide management. It would also shed light on the resource and data points required in managing and documenting these injuries, respectively. With the Active Mobility Bill currently in its infancy, this data could also contribute to the body of evidence underscoring the legislation and provide insights into the role of injury prevention. Therefore, this study aimed to describe the injury patterns sustained by PMD and e-bike users presenting to the emergency department (ED) of a tertiary hospital in Singapore.
METHODS
This retrospective study was conducted on a trauma database of Khoo Teck Puat Hospital, Singapore, from 1 January 2016 to 31 December 2016. The database contained the records of all patients presenting to its ED with trauma as one of the presenting complaints or presentations, and forms part of the Singapore National Trauma Registry (SNTR). The ED had an attendance of 136,976 in 2016, of whom 16.9% (23,094) were trauma patients. All trauma patients who were injured from the use of a PMD or e-bike, or sustained injury as a result of a collision with another user of these mobility devices, were included in this study. Injuries from non-powered (conventional) bicycles and mobility aids (e.g. wheelchairs) were excluded. Patient records with a mechanism of injury coded in the registry as ‘fall’, ‘road traffic accident’ and ‘sports’ were manually hand searched for eligible subjects, as the SNTR did not specifically identify trauma resulting from PMDs and e-bikes.
Information was gathered on patient demographics (age, gender and ethnicity), mode of transport to the ED, type of mobility device used, distribution of injury (based on the nine areas defined in the SNTR), patient acuity category (PAC) scale, injury severity (based on Injury Severity Score [ISS]), resource utilisation (investigation and treatment in the ED, hospitalisation, length of stay, and admission to intensive care unit [ICU]) and cost incurred during ED attendance and hospitalisation. As defined by the Ministry of Health, Singapore, PAC 1 refers to patients needing resuscitation, having cardiovascular collapse or in imminent danger of collapse, or who need to be attended to without a moment’s delay; PAC 2 refers to patients not needing resuscitation, having a major emergency, who are ill and non-ambulatory, or having severe symptoms; and PAC 3 refers to patients with a minor emergency or who are ambulatory with mild to moderate symptoms.
Descriptive statistics of central tendencies were used. The data was further analysed with regard to distribution of injuries according to the types of devices used, injury patterns among minor, moderate and severe injuries, and differences between the injury patterns (collision vs. non-collision impact and motorised vs. non-motorised devices). Data analysis was performed using IBM SPSS Statistics version 22.0 (IBM Corp, Armonk, NY, USA), using chi-square test and Fisher’s exact test as appropriate. A p-value < 0.05 was taken to be statistically significant.
RESULTS
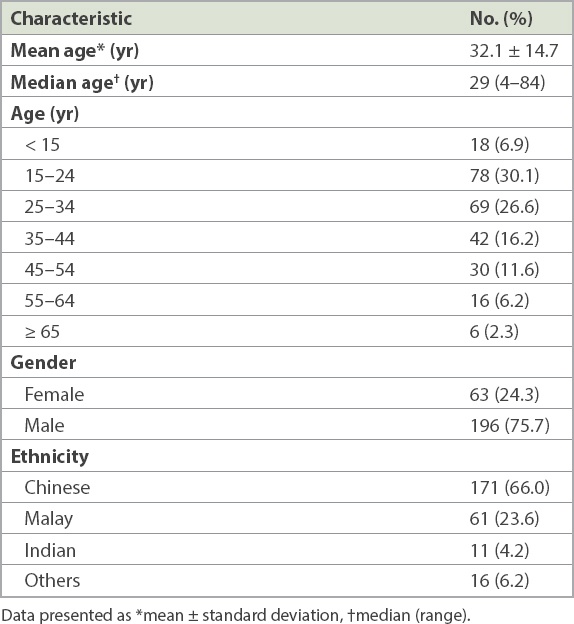
A total of 259 cases were identified during the study period, accounting for 1.1% of the 23,094 trauma patients who were seen in the ED (
Table I
Baseline characteristics of the patients (n = 259).
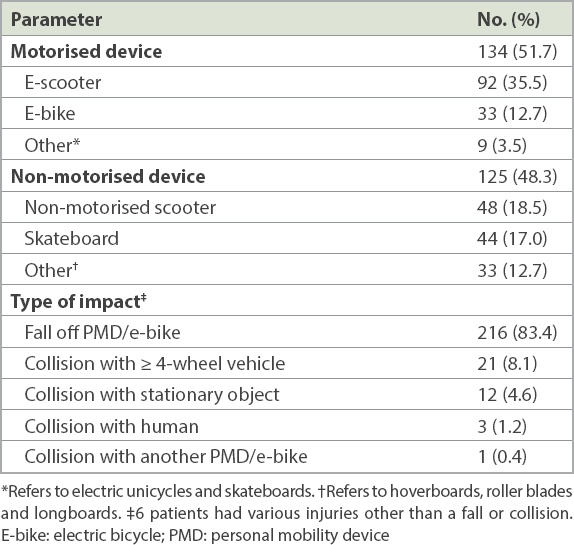
More than half of the patients were injured due to scooters (54.0%), followed by skateboards (17.0%) and motorised bicycles (12.7%) (
Table II
Type of mobility device used and impact.
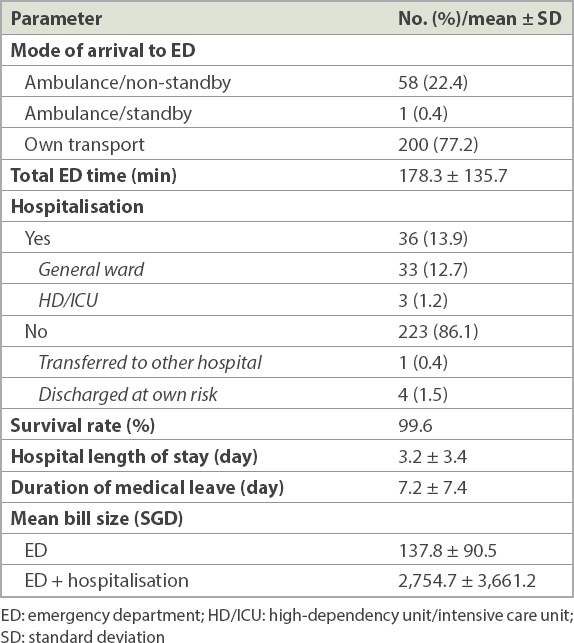
The vast majority of patients arrived at the ED on their own transportation (77.2%) and had an average length of stay of about three hours (
Table III
Processes and outcomes.
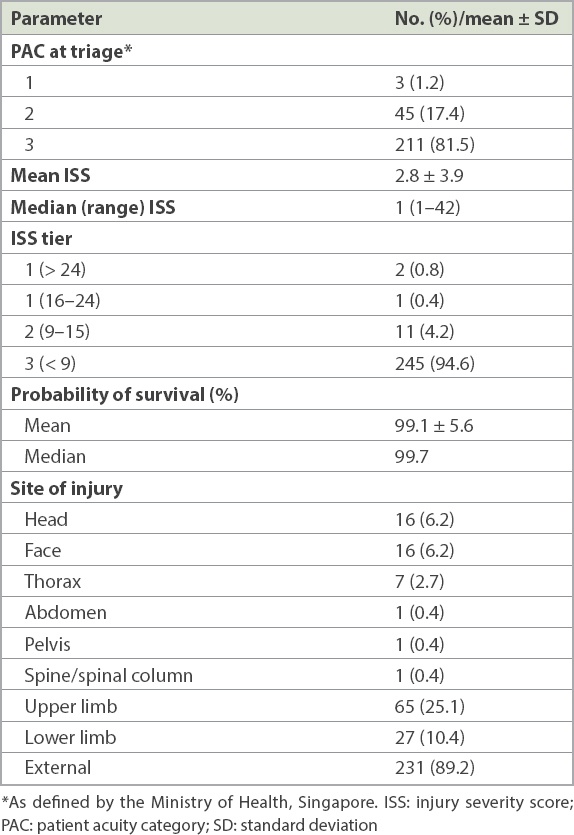
Most patients (81.5%) had minor injuries and were triaged as PAC 3 in the ED (
Table IV
Injury severity and distribution.
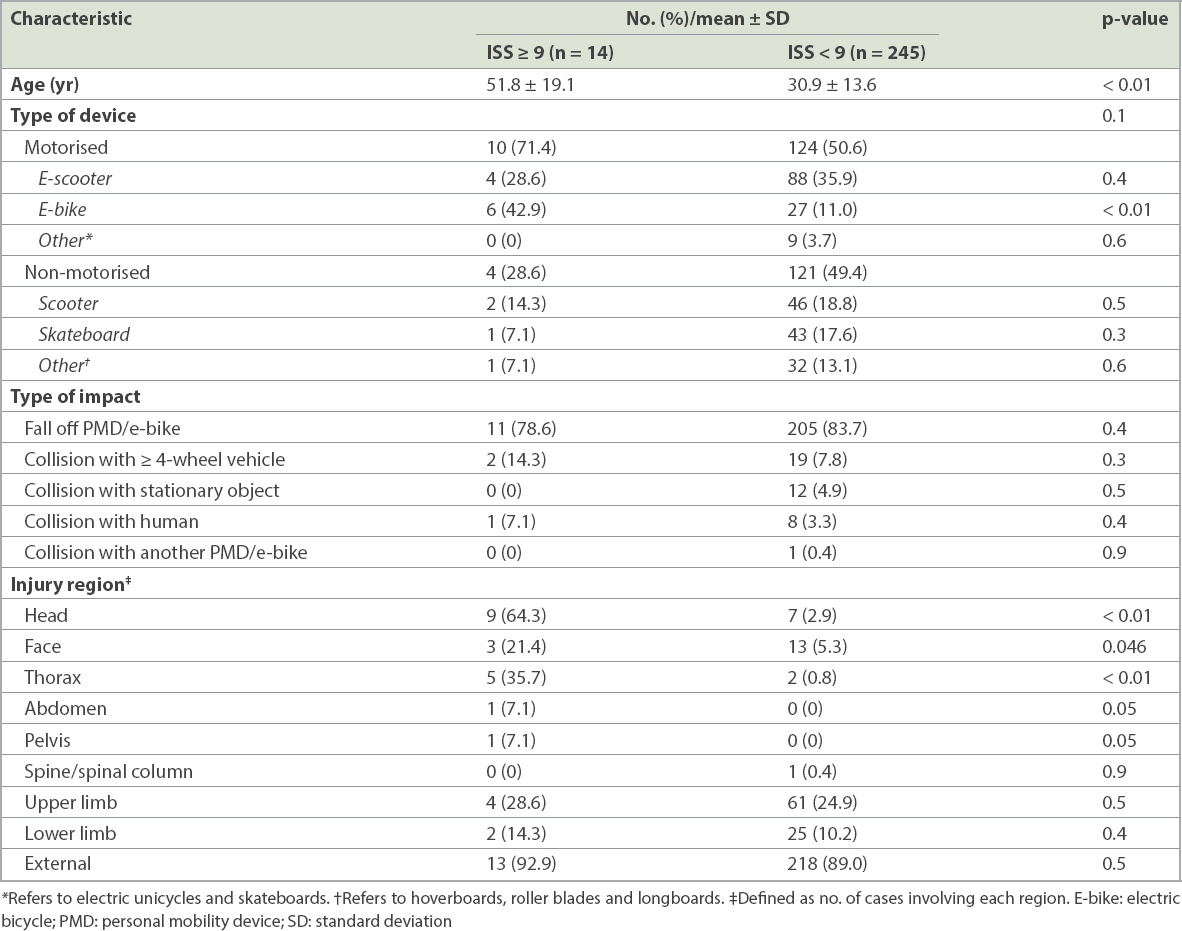
Most of the severe injuries (ISS ≥ 9) were caused by e-bikes (42.9%) and motorised scooters (28.6%) (
Table V
Comparison by injury severity.
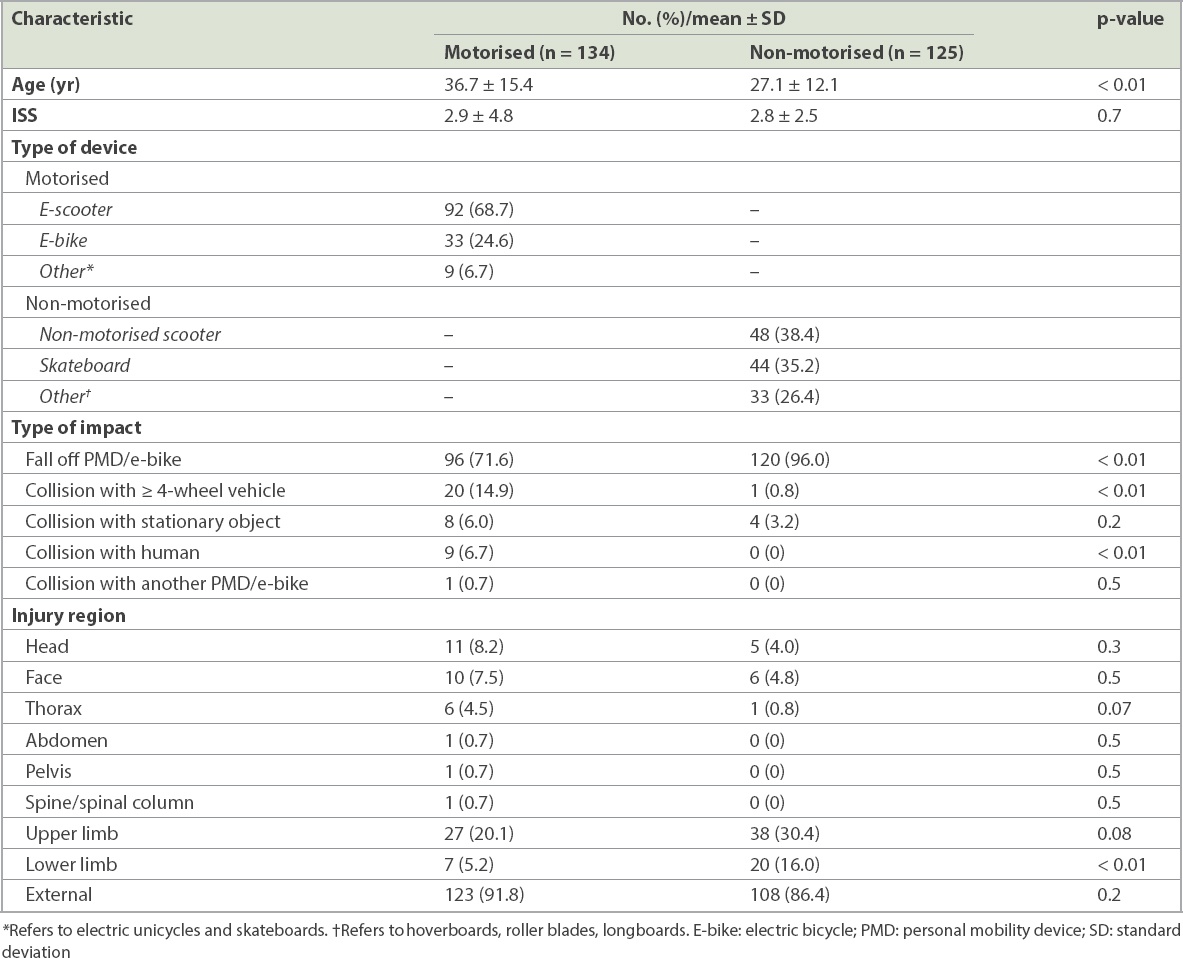
There was no statistical difference between the severity of injuries sustained from motorised devices compared to that from non-motorised devices (
Table VI
Comparison of motorised and non-motorised devices.
DISCUSSION
To the best of our knowledge, this was the first attempt to study injury patterns related to the use of PMDs and e-bikes in Singapore. Most of our injured patients were young, male, and in economically active age groups. The vast majority of the injuries resulted from falls and were mainly treated in an ambulatory setting. Injuries were typically minor, comprising of external wounds or injury to the limbs. This finding is consistent with the general literature.(13)
Compared to patients with minor injuries (ISS < 9), patients with more severe injuries (ISS ≥ 9) tended to be older, with a mean age of 52 years. Severe injuries were also significantly associated with the use of e-bikes (p < 0.01) and with a trend towards the use of motorised mobility devices on the whole, although it did not reach statistical significance (p < 0.1). This finding supports the categorisation of e-bikes separately from other electric PMDs, as put forth by the Active Mobility Bill, and the imposition of tighter regulation compared to other PMDs. Interestingly, it was reported that following the legislation to mandate the registration of e-bikes, the sales of electric scooters increased.(14) Clearly, efforts to promote safer use of PMDs and e-bikes for both users and pedestrians must be collective and concurrent.
Injuries to the head accounted for most of the serious injuries, followed by thoracic and facial injuries, underscoring the importance of helmets for injury prevention. Currently, under the Active Mobility Bill, helmets are only mandatory for e-bike users. However, the use of helmets has been shown to reduce risk of death in both motorised and non-motorised accidents related to the use of recreational vehicles.(15,16) Our research shows the need for greater helmet safety for PMD users as well. On the other hand, abdominal, pelvic and spinal injuries were very uncommon (one patient in each category). This suggests that in a secondary survey of trauma patients using PMDs, emphasis could be paid to the more commonly injured areas of the head, face, limbs and thorax.
Overall, there was no difference in injury severity based on the type of impact (collision vs. non-collision) and type of device used (motorised vs. non-motorised). In a larger registry study involving children between the ages of two and 12 years, Griffin et al found that powered scooter-related injuries were three times more likely to be severe compared to non-powered scooters (odds ratio 3.15, 95% confidence interval 1.87–5.30).(17) The reason for this discrepancy with the literature is unclear and could be related to the smaller sample size of our cohort. However, in the present study, collisions were mostly due to motorised devices (88.4%). This could be due to the greater speed these devices allow. The incident quoted earlier involving the collision of e-scooterist with a car occurred at a zebra crossing.(6) This highlights the importance of PMD and e-bike users physically stopping when approaching pedestrian crossings, looking out for oncoming traffic, and crossing only at walking speed, as spelt out in the code of conduct under the Bill.(8)
Considering the demographics of PMD-related injuries reflected in this study, injury prevention efforts should be targeted at those aged 15–65 years. Attention should also be paid to the Malay community and perhaps the non-Chinese and non-Indian ethnic groups, given their disproportionately higher representation in this cohort. As most injuries were sustained from falling off PMDs and e-bikes, physical conditions such as lighting and the conditions of road and paths, as well as the speed at which these injuries occur, should be evaluated so as to inform injury prevention measures.
Of note, 2.3% of this patient cohort were either pedestrians or pedal cyclists, who were all injured from collision with a motorised PMD. This highlights the potential dangers that PMDs and e-bikes pose to non-PMD users. While rules and a code of conduct are in place for mobility device users, there is also a need to create awareness and educate non-PMD users among the general public about injury prevention measures. Currently, PMDs and conventional bicycles are allowed on footpaths and cycling/shared paths at a speed limit of 15 km/h and 25 km/h, respectively.(10) Other measures such as forbidding the use of e-bikes on footpaths are in keeping with ensuring the safety of pedestrians.
This research is limited in several ways. The data was extracted from a single institution’s trauma database, which could limit its generalisability. Secondly, the current trauma registry dataset does not permit the identification of PMDs and e-bikes as a unique category. This could introduce bias, as hand searching is needed to identify the patient cohort, and it requires detailed documentation of the mechanism of injury by the treating physician. Consequently, the actual incidence of injuries related to PMD and e-bikes could be underestimated. Other relevant data points such as the use of helmets and location (footpath, cycling path or road) where these injuries happen are also not captured in the registry. This would also make it difficult to spot trends in the injuries seen over time and to assess the adequacy and efficacy of current public education efforts and preventive measures. Given the increasing use of PMDs and e-bikes and our research findings, we advocate the creation of a new dataset in the SNTR that is specific to mobility devices.
In conclusion, most injuries sustained by users of PMDs and e-bikes are minor, involving the extremities and external wounds. More severe injuries are associated with the use of e-bikes. This study contributes to the understanding of the injury patterns arising from the use of these new mobility devices in Singapore.