

Dear Sir,
Popliteal artery entrapment syndrome (PAES) is a rare finding whose incidence has been disputed, although it is reportedly more common in female subjects (ratio 2.93:1).(1) Five subtypes are recognised and magnetic resonance angiography (MRA) remains an objective investigation to identify the morphology of PAES.(2,3) We herein present a case of PAES in a patient with calf pain.
A 25-year-old male automated teller machine technician and mixed martial arts (MMA) fighter presented with 12 months of right calf pain. He had no significant medical history and had never smoked. Jogging for five minutes precipitated the cramping pain, leaving him unable to ambulate, but he would recover after 5–10 minutes of rest. His symptoms were significantly limiting his participation in sport.
Clinical examination revealed a diminished right posterior tibial pulse, and symptoms were rapidly reproduced by jogging at 6 km/hr. A repeat peripheral pulse assessment identified an audible popliteal artery bruit but no muscle turgidity. A decreased ankle-brachial pressure index of 0.87 and toe-brachial index of 0.52 was demonstrated in the right leg. The left leg had normal measurements (
Fig. 1
(a) Ankle-brachial pressure index readings show reduced pulse pressures in the right leg from below the knee. There were normal pressures in the left leg. (b) Intraoperative image shows exposed popliteal fossa with the short saphenous vein, sciatic nerve and gastrocnemius muscle.
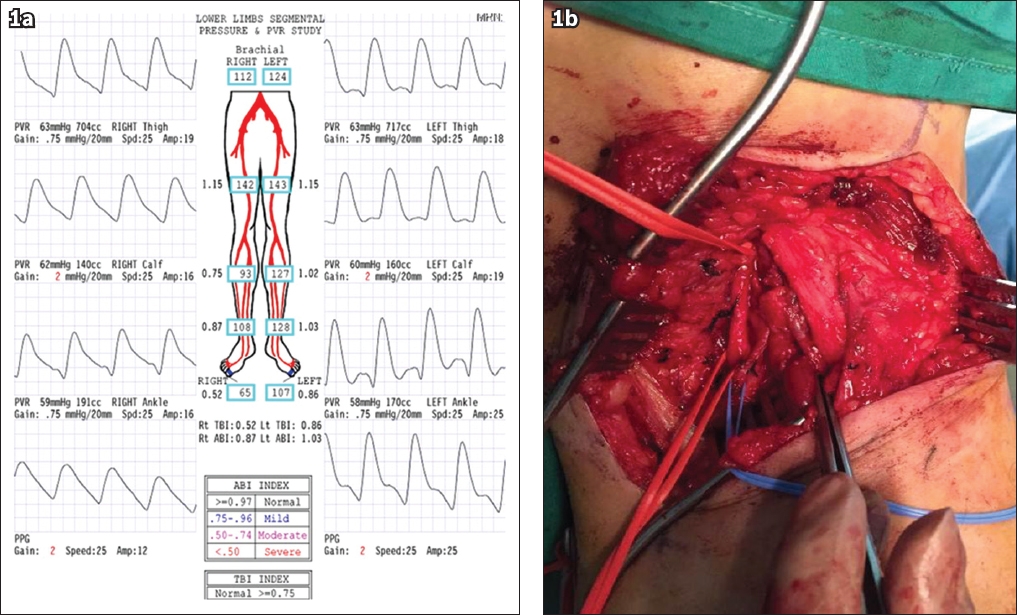
When given a choice between not running and surgery, the patient opted for the latter. Following an incision over the popliteal fossa, the medial head of the gastrocnemius was exposed and its abnormal lateral attachment was resected (
PAES, recognised as a cause of exertional lower leg pain, can have profound consequences such as fibrosis and eventual occlusion of the artery.(4) Thus, it is essential that this problem be identified early from among the other possible causes of exertional leg pain. While this patient experienced unilateral symptoms, bilateral presentations may occur, and the underlying structural anomaly can also differ.(5)
We speculate that the patient’s MMA training programme, which included high-intensity skipping and sparring to strengthen calf muscles, may have contributed to the development of the symptoms. Taking elements from several disciplines, including Muay Thai, wrestling and Brazilian Jujitsu, calf training in MMA helps to maintain an upright posture and a forward weight bias during contests and sparring. This may have induced rapid hypertrophy of the gastrocnemius muscle that, combined with the anomalous popliteal artery position, increased the risk of developing PAES. We urge others to consider this problem in otherwise healthy individuals presenting with chronic exertional leg pain.
Yours sincerely,