Singapore Med J 2021; 62(3): 120-125 doi: https://doi.org/10.11622/smedj.2020021
Unprofessional behaviour of junior doctors: a retrospective analysis of outcomes by the Singapore Medical Council disciplinary tribunals
Norhashirin Binte M Norman1, BRadMedImag(Hons), Joycelyn Mun Peng Soo1, Mathilda Yun Khoon Lam2, T Thirumoorthy3, MBBS, FRCP
Author Information >Copyright and License information >
1Yong Loo Lin School of Medicine, National University of Singapore, Singapore 2Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore 3Duke-NUS Medical School, Singapore Correspondence: Dr T Thirumoorthy, Adjunct Professor, Academic Development Department, Duke-NUS Medical School, 8 College Road, Singapore 169857. gmstt@duke-nus.edu.sg
This is a retrospective analysis of outcomes by Singapore Medical Council (SMC) disciplinary tribunals in cases involving junior doctors. We aimed to classify the types of unprofessional behaviour and consider appropriate measures for remediation and prevention.
METHODS
SMC’s annual reports from 1979 to 2017 and published grounds of decision from 2008 to 2017 were examined using two screening levels to identify cases involving junior doctors. Cases were sorted into five outcome categories: (a) professional misconduct; (b) fraud and dishonesty; (c) defect in character; (d) disrepute to the profession; and (e) acquitted.
RESULTS
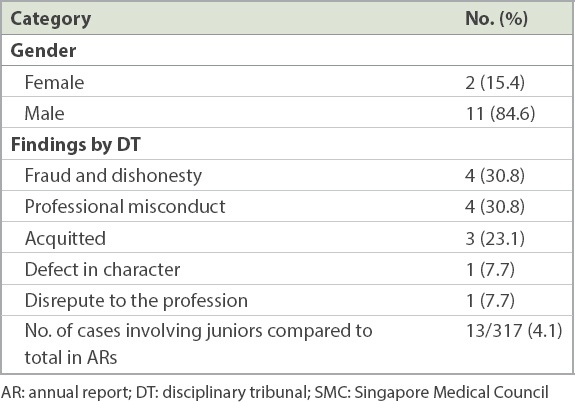
A total of 317 cases were identified, of which 13 (4.1%) involved junior doctors: 4 (30.8%) cases involved professional misconduct, 4 (30.8%) cases involved fraud and dishonesty, 3 (23.1%) cases saw an acquittal, and one case each involved defect in character and disrepute to the profession. The four cases of professional misconduct highlight the need to differentiate medical errors due to systems factors from those due to individual culpability, by applying analytical tools such as root cause analysis and Unsafe Act Algorithms. Disciplining the individual alone does not help prevent the recurrence of similar medical errors. We found that fraud and dishonesty was an important category of unprofessional behaviour among junior doctors.
CONCLUSION
While the frequency of unprofessional behaviour among junior doctors, as determined by the SMC disciplinary tribunal, is low (4.1%), this study highlights that complaints against medical doctors often involve systems issues and individual factors. Unprofessional behaviours related to fraud and dishonesty need special attention in medical school.
Unprofessional behaviour among medical doctors around the world is regulated by disciplinary tribunals (DTs) of medical licensing bodies of the respective country or state of practice. Licensing bodies are increasingly holding doctors to a higher level of professional accountability. The process and outcomes of these disciplinary inquiries have far-reaching impacts on a doctor’s health, career and practice.(1) Professional accountability refers to being called to justify one’s professional actions, behaviours and performance to the various stakeholders in healthcare.(2) The main stakeholders are the patients and their families, through complaints to medical councils. However, due to the complexity of today’s medical practice, doctors can be called to be accountable to hospitals, employers, regulators and even payors.(2)
Over the years, there have been studies on the trends and outcomes of DTs. Most of the literature discussed the risk factors for unprofessional behaviour, types of offences and outcomes of tribunals. There were attempts to categorise the types of unprofessional behaviours, although there is no universally accepted classification.(3-5) A summary of papers from Canada, Australia, New Zealand and the United States (US) showed a higher incidence of disciplinary actions involving family medicine,(6-9) psychiatry,(6-9) and obstetrics and gynaecology.(7-9) Among internal medicine physicians, unprofessional conduct was the commonest offence,(10) while among psychiatrists it was sexual misconduct(11,12) and among anaesthesiologists, standard of care issues.(13)
Several papers in the literature discuss unprofessional behaviours among doctors in training. Resnick et al in 2006 studied US general surgery residents and found that professional misconduct occurs early in training, recurs often and can lead to departure from the training programme.(14) In a literature review of unprofessional behaviour among US medical students and residents, the authors categorised unprofessional behaviour as follows: cheating, misrepresentation of publications, plagiarism, falsification of documents and other dishonest behaviours.(5)
Several papers have discussed the relationship between poor performance during medical school and future disciplinary action taken by medical boards,(15,16) with one reporting that sanctioned doctors are two times more likely to have shown unprofessional conduct in medical school than control doctors.(16) A similar trend was found in doctors who had been sanctioned by the United Kingdom’s General Medical Council – that a history of poor performance in medical school was linked to less likelihood of achieving postgraduate consultant status.(17) Internal medicine physicians in the US who had been sanctioned by state licensing boards were found to have had lower professionalism score ratings in their annual residency evaluation.(18)
The majority of the literature focused on doctors who held independent practice licences and were not under required supervision, such as consultants or doctors in private practice. On average, disciplinary cases involving Canadian doctors occurred around 30 or more years after graduation from medical school,(10,11,19) while doctors from Australia and New Zealand had disciplinary cases an average of 21.4 years after graduation.(7)
We conducted a literature review using the following keywords: (‘disciplined’) and (‘medical doctor’ or ‘physician’ or ‘surgeon’ or ‘resident’ or ‘house officer’ or ‘medical officer’) in the PubMed® and Scopus® databases. The review showed that there is scant literature on the DT outcomes of junior doctors. Furthermore, there were no published papers on outcomes of DTs of doctors in Asia, to the best of our knowledge. To better understand the situation of junior doctors in Singapore, we conducted a study to find out the types of unprofessional behaviour among junior doctors, with the aim of considering appropriate measures for remediation and prevention.
METHODS
We searched the public records of annual reports (ARs) and published grounds of decision (GDs) by the Singapore Medical Council (SMC), the licensing body for medical practitioners in Singapore. Hard copies of the SMC ARs from 1979 to 1999 were retrieved from the National University of Singapore Central Library. Soft copy ARs from 2000 to 2017 and published GDs from 2008 to 2017 were retrieved online from the SMC website.(20,21) Cases regarding health inquiries were excluded. ARs and GDs from the year 2018 were excluded, as they were incomplete at the time of analysis.
Case screening was conducted on two levels. The first was to screen for cases in the ARs and GDs that mentioned the following terms: ‘house officer’ (or ‘houseman’) and ‘medical officer’. The second level of screening involved analysing case text to determine: (a) whether the case happened in a hospital or ambulatory setting (such as general practice), since house officers and medical officers in Singapore typically work in a hospital setting; and (b) if the nature of work reported in the text was descriptive of the work typically done by junior doctors. Cases classified as Level 1 or 2 were included in the study. The cases were then classified into five categories prior to analysis. The categories were adapted from Section 53 of the Medical Registration Act (MRA)(22) and consist of: (a) professional misconduct; (b) fraud and dishonesty; (c) defect in character; (d) disrepute to the profession; (e) acquitted.
RESULTS
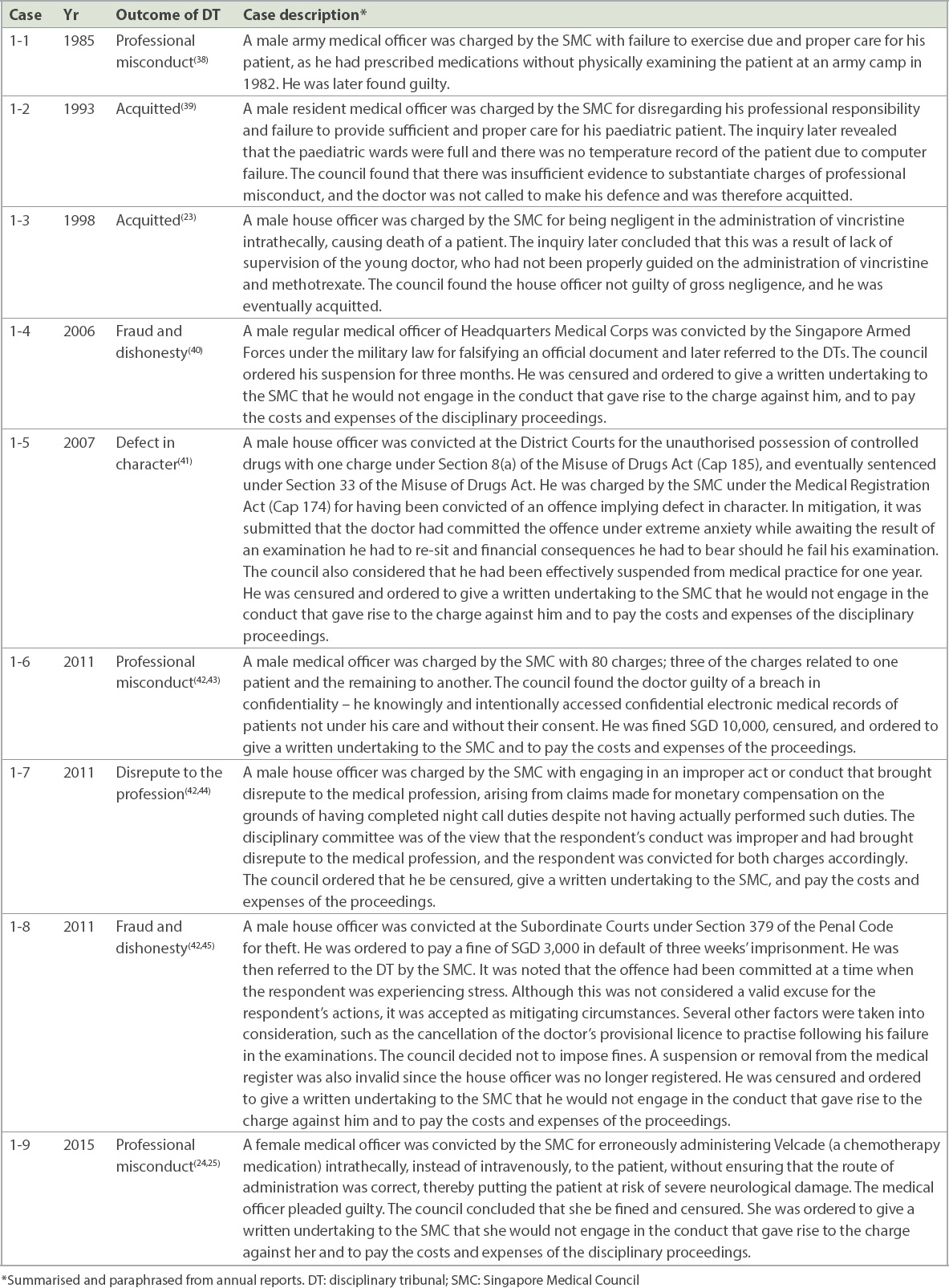
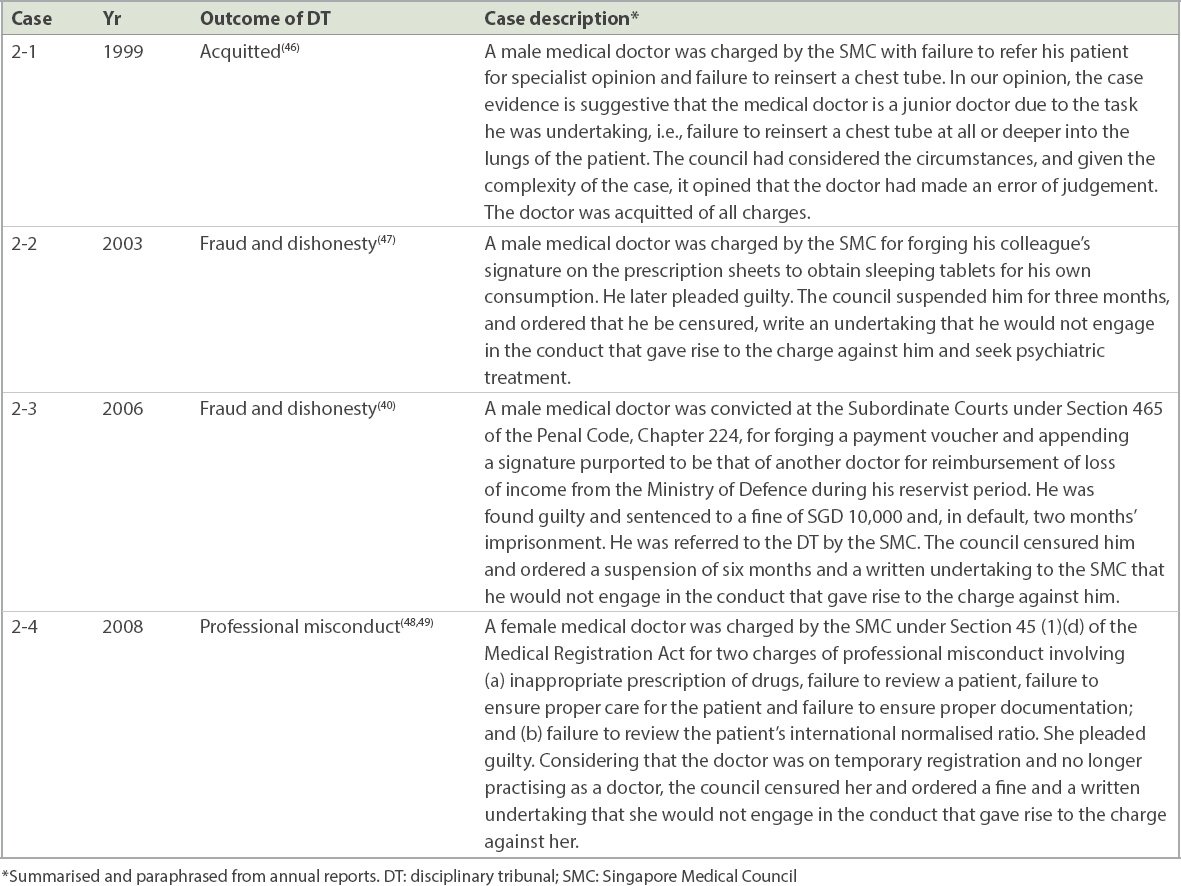
A total of 317 cases were retrieved from the public records of SMC ARs and GDs from 1979 to 2017. Nine cases were identified from the first level of screening (Table I), and four cases were identified from the second level (Table II). Therefore, a total of 13 cases involving junior doctors were identified for analysis, which represents 4.1% of the total number of cases. Table III shows the breakdown of the cases according to categories. Only three doctors were acquitted. Of those sanctioned, the majority of cases (n = 4) involved fraud and dishonesty, followed by professional misconduct (n = 4). One case was identified for each of the categories of defect in character and disrepute to profession.
Table I
Cases involving junior doctors from the first level of screening.
Table II
Cases involving junior doctors from the second level of screening.
Table III
Classification of the 13 cases involving junior doctors.
DISCUSSION
Overall, DT cases involving junior doctors in Singapore make up a very small proportion (4.1%) of the total cases handled by the DT. This is similar to the low rates reported among Canadian medical doctors (seven out of 606 cases, 1%).(6) Among the 13 cases in this study, two categories appeared to be salient, namely professional misconduct (30.8%, n = 4) and fraud and dishonesty (30.8%, n = 4). Two cases involved medical errors with similar contextual features but varying outcomes (Table I, Cases 1-3 & 1-9). These cases, recorded in 1998 and 2015, involved junior doctors who delivered drugs via the wrong route of administration. Case 1-3 occurred in 1998, when a house officer was accused of negligently administering vincristine intrathecally, causing the death of the patient. However, the DT found the doctor not guilty of gross negligence. The justifying points for the verdict were that the doctor was in a very early stage of his housemanship posting (fourth week) and lacked adequate supervision. The doctor was acquitted and the hospital was advised to have closer supervision of doctors in training.(23)
In Case 1-9 in 2015, a medical officer was charged and pleaded guilty. The doctor was censured and fined by the DT for erroneously administering Velcade (bortezomib) intrathecally instead of intravenously to a patient with lymphoma, putting the patient at risk of severe neurological damage.(24,25) The haematology consultant in charge of the patient had ordered chemotherapy, namely intravenous Velcade and intrathecal methotrexate, to be administered to the patient. The intrathecal chemotherapy medication, methotrexate, was to be administered to the patient via lumbar puncture under radiological guidance at the Interventional Radiology Department. When the medical officer arrived at the radiology department, there was only a single syringe containing Velcade. The nurses in the ward had made the mistake of sending down the Velcade injection for the procedure instead of the methotrexate injection.(24) This case clearly illustrates a systems failure medication error. There was a failure to perform ‘jointly double-checking’ (independent checking by two persons of each other) in the administration of ‘high-alert medications’ (drugs that cause significant harm when used in error) at two distinct points: firstly, when the nurse prepared and sent down the Velcade injection, and secondly, when the doctor was injecting the intrathecal drug. In 2015, jointly double-checking was well-known and widely recommended as an essential method to prevent medication errors in cancer chemotherapy.(26)
To highlight the importance of considering systems errors in DTs, we herein discuss a similar case involving a cardiothoracic surgeon.(27) The surgeon was found guilty of professional misconduct by the SMC DT. On appeal, the High Court found that a breakdown of communication and systems failure led to administration of the wrong form of drug, a ‘neat’ cardioplegia solution instead of the diluted form. The High Court overturned the surgeon’s sentence upon appeal, in recognition of the multiple systems factors that contributed to the error and not only the surgeon’s professional conduct and action. These three similar cases heard before the DTs seem to show the persistence of systems error in the administration of high-alert drugs to patients. Addressing systems issues using the punitive approach alone does not resolve any systems issues, instead allowing any inherent weaknesses in the system to persist and the error to recur.(28)
Medical errors are a result of a combination of active failures of the healthcare professional and latent conditions of the system.(29,30) Active failures refer to human errors such as slips, lapses, fumbles and procedural violations committed by those in direct contact with the patient.(31) Latent conditions refer to system design decisions made at different levels from builders to management, which create a high-risk environment for errors.(31) Root cause analysis can be used to differentiate between active failures and latent conditions.
Healthcare professionals should be empowered to report errors in the system while also being accountable for their own actions. This is encapsulated in the concept of ‘just culture’, which advocates balancing the accountability of healthcare workers and improving innate systems errors as an approach to improving patient safety.(28) The main challenge in medical error analysis is differentiating between active failures and errors from latent conditions.(28) Active errors can then be subjected to the Unsafe Acts Algorithm, as proposed by Leonard and Frankel, to determine if the acts are intentional, reckless or malicious, as opposed to unintentional.(32) Marx(33) recommends that intentional, reckless and malicious acts should be recognised and punished, whereas unintentional and systems error require coaching and remediation. The challenge lies in constructing instruments and regulations to objectively classify each case into these distinct categories.
Effective and just management of professional misconduct must not solely focus on punishing those who have made a mistake. Instead, we should work towards remediating the behaviour of those who have done wrong, such that these mistakes are not repeated. At the same time, system errors need to be recognised and corrected. Four cases in this study had the verdict of fraud and dishonesty. These involved falsifying official documents (including a prescription for sleeping pills) and theft. In a survey of graduating medical students, up to 24% (range 13%–24%) of students admitted to dishonest behaviours during clinical clerkships.(34) These included recording tasks that they did not actually perform in medical records or lying about ordering tests when they had not done so. The authors’ explanation was that dishonest behaviours were culturally pervasive and acceptable because no one was directly harmed.(34) In a focus group study in South Korea, a strong workplace hierarchical culture was noted as a cause for resident misbehaviour and the propagation of dishonest practices.(3) The reasons for such behaviour involved concerns about the adverse consequences of being truthful; in particular, fear of being blamed and shamed, and unreasonable response and demands by a senior colleague who might not understand the juniors’ disposition. Professional burnout among medical students(35) and residents(5) increases the risk of engaging in cheating and dishonest clinical behaviours.
It is interesting to note that in these cases of fraud and dishonesty, the incidents occurred outside the doctor-patient relationship. We believe that these dishonest actions can be attributed to the doctors’ ignorance and failure to recognise that behaviours outside of professional work will impact their medical professional standing and career. Hence, it is vital that medical students are made to recognise from the beginning that a doctor’s work requires the public’s trust, and that they are held to higher ethical and legal standards compared to the rest of the population.(36) Dishonest behaviours and actions not only have serious ethical implications and attract disciplinary repercussions for the doctor, but most importantly, undermine the trust patients have in the medical profession.
We recommend using these cases we have highlighted from the SMC’s ARs and GDs as case studies in medical schools. Medical students should be enculturated in the clinical environment to truly understand the importance of the integrity and honesty that are required of the medical profession. Other points worth highlighting from this study are regarding the health and wellness of medical students and junior doctors. Psychosocial difficulties such as psychiatric illness, substance abuse, and family and relationship issues are reported to be factors contributing to the offences (Table I, Cases 1-5 & 1-8). Hence, greater resources should be mobilised to promote student/resident wellness and health in the workplace.(37)
In conclusion, the frequency of unprofessional behaviour that is referred to the DT and involves junior doctors in Singapore is considerably low at only 13 cases, making up approximately 4.1% of the DT proceedings. This study highlights that complaints against medical doctors often involve both human factors and deeper systems issues within the workplace environment. Instruments such as root cause analysis and the Unsafe Act Algorithm(32,33) should be applied to differentiate between blameworthy actions and blameless acts resulting from systems issues. Malicious and reckless behaviour of individuals that is intentional and deliberate requires an appropriate disciplinary process. Taking appropriate measures to correct systems issues, instead of a merely punitive approach, helps to prevent medical errors. To address unprofessional behaviours among junior doctors, case studies should be used in formal education to increase awareness of such offences among medical students and trainees and to emphasise the high professional standard required of the medical profession. Better support networks for junior doctors should be implemented, making it a priority to address personal and mental health issues.
References Verhoef LM, Weenink JW, Winters S, et al. The disciplined healthcare professional: a qualitative interview study on the impact of the disciplinary process and imposed measures in the Netherlands.BMJ Open. 2015;5:e009275. Deber RB.Thinking about accountability.Healthc Policy. 2014;10:12-24. Chang HJ, Lee YM, Lee YH, Kwon HJ.Investigation of unethical and unprofessional behavior in Korean residency training.Teach Learn Med. 2015;27:370-8. Teherani A, Hodgson CS, Banach M, Papadakis MA.Domains of unprofessional behavior dang medical school associated with future disciplinary action by a state medical board.Acad Med. 2005;80:10 SupplS17-20. Fargen KM, Drolet BC, Philibert I.Unprofessional behaviors among tomorrow's physicians: review of the literature with a focus on risk factors, temporal trends, and future directions.Acad Med. 2016;91:858-64. Alam A, Klemensberg J, Griesman J, Bell CM.The characteristics of physicians disciplined by professional colleges in Canada.Open Med. 2011;5:e166-72. Elkin KJ, Spittal MJ, Elkin DJ, Studdert DM.Doctors disciplined for professional misconduct in Australia and New Zealand, 2000-2009.Med J Aust. 2011;194:452-6. Khaliq AA, Dimassi H, Huang CY, Narine L, Smego RA, JrlastDisciplinary action against physicians:who is likely to get disciplined?.Am J Med. 2005;118:773-7. Kohatsu ND, Gould D, Ross LK, Fox PJ.Characteristics associated with physician discipline:a case-control study.Arch Intern Med. 2004;164:653-8. Liu JJ, Alam AQ, Goldberg HR, Matelski JJ, Bell CM.Characteristics of internal medicine physicians disciplined by professional colleges in Canada.Medicine (Baltimore). 2015;94:e937. Alam A, Kurdyak P, Klemensberg J, Griesman J, Bell CM.The characteristics of psychiatrists disciplined by professional colleges in Canada.PLoS One. 2012;7:e50558. Morrison J, Morrison T.Psychiatrists disciplined by a state medical board.Am J Psychiatry. 2001;158:474-8. Alam A, Khan J, Liu J, et al. Characteristics and rates of disciplinary findings amongst anesthesiologists by professional colleges in Canada.Can J Anaesth. 2013;60:1013-9. Resnick AS, Mullen JL, Kaiser LR, Morris JB.Patterns and predictions of resident misbehavior--a 10-year retrospective look.Curr Surg. 2006;63:418-25. Papadakis MA, Hodgson CS, Teherani A, Kohatsu ND.Unprofessional behavior in medical school is associated with subsequent disciplinary action by a state medical board.Acad Med. 2004;79:244-9. Papadakis MA, Teherani A, Banach MA, et al. Disciplinary action by medical boards and prior behavior in medical school.N Engl J Med. 2005;353:2673-82. Yates J, James D.Risk factors at medical school for subsequent professional misconduct: multicentre retrospective case-control study.BMJ. 2010;340:c2040. Papadakis MA, Arnold GK, Blank LL, Holmboe ES, Lipner RS.Performance dang internal medicine residency training and subsequent disciplinary action by state licensing boards.Ann Intern Med. 2008;148:869-76. Alam A, Matelski JJ, Goldberg HR, et al. The characteristics of international medical graduates who have been disciplined by professional regulatory colleges in Canada:a retrospective cohort study.Acad Med. 2017;92:244-9. Singapore Medical CouncilSMC Annual Reports. Available at: http://www.healthprofessionals.gov.sg/smc/publications-newsroom/smc-annual-reports. Accessed August 31, 2018. Singapore Medical CouncilPublished Grounds of Decisions. Available at: http://www.healthprofessionals.gov.sg/smc/published-grounds-of-decision. Accessed September 16, 2018. Medical Registration Act (Chapter 174)Singapore Statutes Online [online]. Available at: https://sso.agc.gov.sg/Act/MRA1997. Accessed September 16, 2018. Singapore Medical CouncilDisciplinary Inquiries - Negligence in Administering Vincristine Intrathecally:Case 7.Singapore Medical Council Annual Report 1998. 1998;Singapore The Council16-7. Singapore Medical Council Disciplinary Tribunal Inquiry for Dr Garuna Murthee Kavitha held on 21 April 2015. Available at: http://www.healthprofessionals.gov.sg/docs/librariesprovider2/published-grounds-of-decision/year-2015/dr-garuna-kavitha-(150421).pdf. Accessed September 16, 2018. Singapore Medical CouncilProfessional Negligence/Incompetence. Case 6:Dr Garuna Murthee Kavitha.Annual Report. 2015;Accessed September 16, 201827-8. Available at: https://www.healthprofessionals.gov.sg/docs/librariesprovider2/publications-newsroom/smc-annual-reports/smc-annual-report-2015.pdf. Accessed September 16, 2018. Schwappach DL, Pfeiffer Y, Taxis K.Medication double-checking procedures in clinical practice:a cross-sectional survey of oncology nurses'experiences.BMJ Open. 2016;6:e011394. Uwe Klima v.Singapore Medical Council [2015] SGHC 97.. Available at: https://www.singaporelawwatch.sg/Portals/0/Docs/Judgments/[2015]%20SGHC%2097.pdf. Accessed January 1, 2019. Boysen PG, 2ndlastJust culture:a foundation for balanced accountability and patient safety.Ochsner J. 2013;13:400-6. Reason J.Reason J.Latent errors and systems disasters.Human Error. 1990;Cambridge Cambridge University Press173-216. Reason J.Human Error.. 1990;Cambridge Cambridge University Press. Reason J.Human error:models and management.BMJ. 2000;320:768-70. Leonard MW, Frankel A.The path to safe and reliable healthcare.Patient Educ Couns. 2010;80:288-92. Marx D.Patient Safety and the “Just Culture”:A Primer for Health Care Executives.. 2001;City of New York Trustees of Columbia University. Dans PE.Self-reported cheating by students at one medical school.Acad Med. 1996;71:1 SupplS70-2. Dyrbye LN, Massie FS, JrEacker A, et al. Relationship between burnout and professional conduct and attitudes among US medical students.JAMA. 2010;304:1173-80. Menon S.Medicine and law:comparative perspectives on professional conduct and discipline.Academy of Medicine - Singapore's Professional Affairs Lecture. Available at: https://www.annals.edu.sg/PDF/SundareshMenon/LectureCJMarch2018_2.pdf. Accessed September 16, 2018. Reamy BV, Harman JH.Residents in trouble:an in-depth assessment of the 25-year experience of a single family medicine residency.Fam Med. 2006;38:252-7. Singapore Medical CouncilDisciplinary Inquiries Held in 1985 - Summary of Findings [Case No. 2].Singapore Medical Council Annual Report 1985. 1985;Singapore The Council10. Singapore Medical CouncilDisciplinary Inquiries Held in 1993 - Summary and Findings [Case:Failure to Provide Immediate Medical Attention to an 8-month-old Baby].Singapore Medical Council Annual Report 1993. 1993;Singapore The Council10. Singapore Medical CouncilDisciplinary Inquiries Held in 2006. Conviction in Court. Cases 3 and 4.Singapore Medical Council Annual Report. 2006;Accessed September 16, 201820-1. Available at: https://www.healthprofessionals.gov.sg/docs/librariesprovider2/publications-newsroom/smc-annual-reports/smc-annual-report-2006.pdf. Accessed September 16, 2018. Singapore Medical CouncilDisciplinary Inquiries Held in 2007. Conviction in Court. Case 8.Singapore Medical Council Annual Report. 2007;Accessed September 16, 201821-2. Available at: https://www.healthprofessionals.gov.sg/docs/librariesprovider2/publications-newsroom/smc-annual-reports/annual-report-v06.pdf. Accessed September 16, 2018. Singapore Medical CouncilProfessional misconduct in patient management. Cases 5, 6 and 11.Singapore Medical Council Annual Report. 2011;Accessed September 16, 201827-8. Available at: https://www.healthprofessionals.gov.sg/docs/librariesprovider2/publications-newsroom/smc-annual-reports/smc-annual-report-2011_for-website.pdf. Accessed September 16, 2018. Singapore Medical Council Disciplinary Committee Inquiry for Dr Singh Tregon Randhawa Held on 28 and 29 November 2011. Available at: http://www.healthprofessionals.gov.sg/docs/librariesprovider2/published-grounds-of-decision/year-2012/dr-singh-tregon-randhawa.pdf?sfvrsn=2cbbb629_0. Accessed September 16, 2018. Singapore Medical Council Disciplinary Committee Inquiry for Dr Ho Mien Held on 21 July 2010, 15 August 2011, 22 August 2011 and 16 December 2011. Available at: https://www.healthprofessionals.gov.sg/docs/librariesprovider2/published-grounds-of-decision/year-2012/dr-ho-mien.pdf?sfvrsn=5b2bd9b5_0. Accessed September 16, 2018. Singapore Medical Council Disciplinary Committee Inquiry for Dr Quah Weiren Charles Abraham on 27 May 2011. Available at: http://www.healthprofessionals.gov.sg/docs/librariesprovider2/published-grounds-of-decision/year-2011/00-sentence-and-verdict---dr-quah-weiren-(110527)---for-website.pdf?sfvrsn=5d3eb49a_0. Accessed September 16, 2018. Singapore Medical CouncilDisciplinary Inquiries Held in 1999 - Negligence in the Treatment of the Patient [Case 12].Singapore Medical Council Annual Report 1999. 1999;Singapore The Council18. Singapore Medical CouncilDisciplinary Inquiries Held in 2003. Forgery:Case 5.Singapore Medical Council Annual Report 2003. Available at: https://www.healthprofessionals.gov.sg/docs/librariesprovider2/publications-newsroom/smc-annual-reports/annual-report-2003.pdf. Accessed September 16, 2018. Singapore Medical CouncilExcessive/inappropriate prescription of drugs (non-Subutex):Case 5.Singapore Medical Council Annual Report 2008:20. Available at: https://www.healthprofessionals.gov.sg/docs/librariesprovider2/publications-newsroom/smc-annual-reports/smc-annual-report-2008-(final-printed-version).pdf. Accessed September 16, 2018. Singapore Medical Council Disciplinary Inquiry against Dr AAJ Held on 11 November 2008. Available at: https://www.healthprofessionals.gov.sg/docs/librariesprovider2/published-grounds-of-decision/year-2008/dr-aaj-(2008)---grounds-of-decision.pdf?sfvrsn=60b62a82_0. Accessed September 16, 2018.
REFERENCES:
1. Verhoef LM, Weenink JW, Winters S, et al. The disciplined healthcare professional: a qualitative interview study on the impact of the disciplinary process and imposed measures in the Netherlands. BMJ Open 2015; 5:e009275. https://doi.org/10.1136/bmjopen-2015-009275
PMid:26608639 PMCid:PMC4663436
3. Chang HJ, Lee YM, Lee YH, Kwon HJ. Investigation of unethical and unprofessional behavior in Korean residency training. Teach Learn Med 2015; 27:370-8. https://doi.org/10.1080/10401334.2015.1077128
PMid:26507994
4. Teherani A, Hodgson CS, Banach M, Papadakis MA. Domains of unprofessional behavior during medical school associated with future disciplinary action by a state medical board. Acad Med 2005; 80(10 Suppl):S17-20. https://doi.org/10.1097/00001888-200510001-00008
PMid:16199450
5. Fargen KM, Drolet BC, Philibert I. Unprofessional behaviors among tomorrow's physicians: review of the literature with a focus on risk factors, temporal trends, and future directions. Acad Med 2016; 91:858-64. https://doi.org/10.1097/ACM.0000000000001133
PMid:26910897
6. Alam A, Klemensberg J, Griesman J, Bell CM. The characteristics of physicians disciplined by professional colleges in Canada. Open Med 2011; 5:e166-72.
7. Elkin KJ, Spittal MJ, Elkin DJ, Studdert DM. Doctors disciplined for professional misconduct in Australia and New Zealand, 2000-2009. Med J Aust 2011; 194:452-6. https://doi.org/10.5694/j.1326-5377.2011.tb03058.x
PMid:21534900
8. Khaliq AA, Dimassi H, Huang CY, Narine L, Smego RA Jr. Disciplinary action against physicians: who is likely to get disciplined? Am J Med 2005; 118:773-7. https://doi.org/10.1016/j.amjmed.2005.01.051
PMid:15989912
9. Kohatsu ND, Gould D, Ross LK, Fox PJ. Characteristics associated with physician discipline: a case-control study. Arch Intern Med 2004; 164:653-8. https://doi.org/10.1001/archinte.164.6.653
PMid:15037494
10. Liu JJ, Alam AQ, Goldberg HR, Matelski JJ, Bell CM. Characteristics of internal medicine physicians disciplined by professional colleges in Canada. Medicine (Baltimore) 2015; 94:e937. https://doi.org/10.1097/MD.0000000000000937
PMid:26131839 PMCid:PMC4504618
11. Alam A, Kurdyak P, Klemensberg J, Griesman J, Bell CM. The characteristics of psychiatrists disciplined by professional colleges in Canada. PLoS One 2012; 7:e50558. https://doi.org/10.1371/journal.pone.0050558
PMid:23209779 PMCid:PMC3509088
12. Morrison J, Morrison T. Psychiatrists disciplined by a state medical board. Am J Psychiatry 2001; 158:474-8. https://doi.org/10.1176/appi.ajp.158.3.474
PMid:11229991
13. Alam A, Khan J, Liu J, et al. Characteristics and rates of disciplinary findings amongst anesthesiologists by professional colleges in Canada. Can J Anaesth 2013; 60:1013-9. https://doi.org/10.1007/s12630-013-0006-8
PMid:23897490
14. Resnick AS, Mullen JL, Kaiser LR, Morris JB. Patterns and predictions of resident misbehavior--a 10-year retrospective look. Curr Surg 2006; 63:418-25. https://doi.org/10.1016/j.cursur.2006.05.004
PMid:17084771
15. Papadakis MA, Hodgson CS, Teherani A, Kohatsu ND. Unprofessional behavior in medical school is associated with subsequent disciplinary action by a state medical board. Acad Med 2004; 79:244-9. https://doi.org/10.1097/00001888-200403000-00011
PMid:14985199
16. Papadakis MA, Teherani A, Banach MA, et al. Disciplinary action by medical boards and prior behavior in medical school. N Engl J Med 2005; 353:2673-82. https://doi.org/10.1056/NEJMsa052596
PMid:16371633
17. Yates J, James D. Risk factors at medical school for subsequent professional misconduct: multicentre retrospective case-control study. BMJ 2010; 340:c2040. https://doi.org/10.1136/bmj.c2040
PMid:20423965 PMCid:PMC3191727
18. Papadakis MA, Arnold GK, Blank LL, Holmboe ES, Lipner RS. Performance during internal medicine residency training and subsequent disciplinary action by state licensing boards. Ann Intern Med 2008; 148:869-76. https://doi.org/10.7326/0003-4819-148-11-200806030-00009
PMid:18519932
19. Alam A, Matelski JJ, Goldberg HR, et al. The characteristics of international medical graduates who have been disciplined by professional regulatory colleges in Canada: a retrospective cohort study. Acad Med 2017; 92:244-9. https://doi.org/10.1097/ACM.0000000000001356
PMid:27603039
22. Medical Registration Act (Chapter 174). In: Singapore Statutes Online [online]. Available at: https://sso.agc.gov.sg/Act/MRA1997. Accessed September 16, 2018.
23. Singapore Medical Council. Disciplinary Inquiries - Negligence in Administering Vincristine Intrathecally: Case 7. In: Singapore Medical Council Annual Report 1998. Singapore: The Council, 1998: 16-7.
26. Schwappach DL, Pfeiffer Y, Taxis K. Medication double-checking procedures in clinical practice: a cross-sectional survey of oncology nurses' experiences. BMJ Open 2016; 6:e011394. https://doi.org/10.1136/bmjopen-2016-011394
PMid:27297014 PMCid:PMC4916573
28. Boysen PG 2nd. Just culture: a foundation for balanced accountability and patient safety. Ochsner J 2013; 13:400-6.
29. Reason J. Latent errors and systems disasters. In: Reason J, ed. Human Error. Cambridge: Cambridge University Press; 1990: 173-216. https://doi.org/10.1017/CBO9781139062367.008
30. Reason J. Human Error. Cambridge: Cambridge University Press; 1990.
35. Dyrbye LN, Massie FS Jr, Eacker A, et al. Relationship between burnout and professional conduct and attitudes among US medical students. JAMA 2010; 304:1173-80. https://doi.org/10.1001/jama.2010.1318
PMid:20841530
36. Menon S. Medicine and law: comparative perspectives on professional conduct and discipline. In: Academy of Medicine - Singapore's Professional Affairs Lecture. Available at: https://www.annals.edu.sg/PDF/SundareshMenon/LectureCJMarch2018_2.pdf. Accessed September 16, 2018.
37. Reamy BV, Harman JH. Residents in trouble: an in-depth assessment of the 25-year experience of a single family medicine residency. Fam Med 2006; 38:252-7.
38. Singapore Medical Council. Disciplinary Inquiries Held in 1985 - Summary of Findings [Case No. 2]. In: Singapore Medical Council Annual Report 1985. Singapore: The Council, 1985: 10.
39. Singapore Medical Council. Disciplinary Inquiries Held in 1993 - Summary and Findings [Case: Failure to Provide Immediate Medical Attention to an 8-month- old Baby]. Singapore Medical Council Annual Report 1993. Singapore: The Council, 1993: 10.
46. Singapore Medical Council. Disciplinary Inquiries Held in 1999 - Negligence in the Treatment of the Patient [Case 12]. Singapore Medical Council Annual Report 1999. Singapore: The Council, 1999: 18.